



Table of Contents
Quick Answer: Can You Run With Prolapse?
Yes, even with prolapse, you can absolutely return to running, lifting weights, jumping, and participating in the activities you enjoy. A prolapse diagnosis does not automatically mean you need to stop exercising or avoid impact forever. While returning to running with prolapse often requires rebuilding strength, improving pressure management, and gradually reintroducing impact, many have successfully returned to everything from recreational running to marathons and endurance events.
If you’re looking for a place to start, grab our Free Pelvic Floor Exercise Guide. It includes some of our favorite mobility, breathing, and strengthening exercises that can help support pelvic floor function and improve your body’s ability to manage pressure.
Our Return to Racing After Four Babies
Last weekend was a special milestone for our family. My sister, Roxanne, completed her first 10K since giving birth to her fourth baby just five months ago. Not only did she finish feeling strong, but she also completed the race without experiencing prolapse symptoms. I ran the race alongside her, and as someone who also has prolapse after birth, it was a meaningful reminder that a diagnosis does not automatically determine what you are capable of doing.
Our next challenge is already on the calendar. This fall, we’ll be tackling a race weekend that includes a 5K, 10K, and half marathon over three days. While that goal may seem far away if you’re newly postpartum or navigating a prolapse diagnosis, we wanted to share some of the strategies that have helped both of us continue running and training after childbirth.
Why This Topic Matters So Much to Me
After the birth of my first baby, I felt incredibly lost. Before becoming a mom, I was an Army officer, a collegiate runner, an ultramarathon runner, and a member of the Army Ten-Miler team at Fort Bragg. Running wasn’t just exercise for me. It was a significant part of my identity, and when I left my full-time career and became a stay-at-home mom, I found myself trying to figure out who I was outside of motherhood.
One of the things that helped me reconnect with myself was running. In fact, the very first program I created for MamasteFit was our Postpartum Return to Running Program because I was trying to figure out how to safely rebuild after childbirth. What started as stroller walks and short run-walk intervals eventually helped me return to racing, and years later, I used many of those same principles to run a sub-four-hour marathon nine months postpartum and continue training for races today.
Because of that experience, I am incredibly passionate about helping women understand that a prolapse diagnosis does not automatically mean the end of an active lifestyle. I’ve now worked with hundreds of women through pregnancy and postpartum, and one of the most common fears I hear is that they’ll never be able to run again. Fortunately, that is rarely the case.
Prolapse 101: What Is It, Myths, and Symptoms
In the first part of this blog, I want to address some common myths and misunderstandings about prolapse. There is a lot of fear associated with a prolapse diagnosis, and you may feel overwhelmed, helpless, or confused about what you’re supposed to do next. You may even have been told to stop running, lifting, jumping, or participating in activities you enjoy.
The good news is that many of the messages surrounding prolapse are outdated, overly restrictive, or simply not supported by clinical evidence. Before we talk about how we approach prolapse, pelvic floor balance, and returning to running, let’s start by clearing up some of the biggest misconceptions.
First, Let’s Talk About Some Prolapse Myths
One of the biggest misconceptions surrounding prolapse is that a diagnosis means you need to stop being active. Many are told to avoid running, jumping, lifting heavy weights, or participating in high-impact exercise after discovering they have prolapse. Unfortunately, this advice is often given without much discussion of symptoms, function, training history, goals, or the many factors that influence pelvic floor health.
At MamasteFit, we take a different approach. We have worked with countless women who have successfully returned to running, strength training, CrossFit, recreational sports, and endurance events after a prolapse diagnosis. You can have prolapse and run. You can have prolapse and lift weights. You can have prolapse and have additional children. You can even have prolapse after a C-section. The goal is not to avoid movement, but rather to learn how to support your body so you can continue participating in the activities that matter to you.
A Prolapse Diagnosis Does Not Always Mean There Is a Functional Problem
One challenge with prolapse diagnoses is that most women never had their pelvic floor assessed before pregnancy. Because of this, we often have no idea what our pelvic organ support looked like before having children. While pregnancy and childbirth absolutely increase the risk of prolapse, it can be difficult to know exactly how much of our current presentation developed during pregnancy versus what may have already existed within our individual anatomy.
In fact, research has shown that some degree of pelvic organ prolapse exists even among women who have never given birth. A 2022 study of vaginally nulliparous women found that nearly 30% demonstrated clinically significant prolapse on examination, despite never having delivered vaginally. This doesn’t mean pregnancy and birth don’t matter. They absolutely do. It simply reminds us that pelvic organ support exists on a spectrum and that childbirth is only one piece of a much larger picture that includes genetics, connective tissue characteristics, age, pressure management, and overall pelvic floor function.
This is one reason we encourage women to focus on symptoms and function rather than becoming overly focused on a specific prolapse grade. The position of your pelvic organs is only one piece of the puzzle. How your body functions matters significantly more than what a single assessment reveals.
A comparison I often make is the changes we see in our skin after pregnancy. Many of us have looser skin postpartum than we did before having children. Our bodies may look different, but that does not automatically mean something is wrong. Similarly, some women may have pelvic organs that naturally sit a little lower than those of others, yet experience no symptoms or limitations in their daily lives.
Interestingly, research has also shown that symptoms and prolapse stage do not always correlate particularly well. In other words, someone with a more significant prolapse on examination may have very few symptoms, while someone with a less significant prolapse may feel much more bothered by it. This is why we spend so much time focusing on function, movement, symptom management, and quality of life rather than becoming overly attached to a specific prolapse grade.
If you have prolapse but do not experience symptoms, that is often a sign that your body is functioning quite well. You can have prolapse and live an active life. You can have prolapse and run races. You can have prolapse and lift weights. A diagnosis alone does not determine what you are capable of doing.
Symptoms Often Fluctuate, and That’s Normal
Even when symptoms are present, they are rarely perfectly linear. Roxanne recently completed her first postpartum 10K after her fourth baby without experiencing prolapse symptoms during the race. I have also continued running and strength training with prolapse. Yet despite feeling strong and capable, there are still days when I notice more symptoms than others, even nearly two years postpartum.
This does not necessarily mean the prolapse has worsened. Symptoms often fluctuate with sleep, stress, recovery, constipation, training volume, hydration status, hormonal changes, and how we manage pressure throughout the day. One of the most helpful mindset shifts is learning to view symptoms as information rather than viewing them as proof that something is wrong. Symptoms can help guide training decisions and recovery strategies without necessarily indicating that damage has occurred.
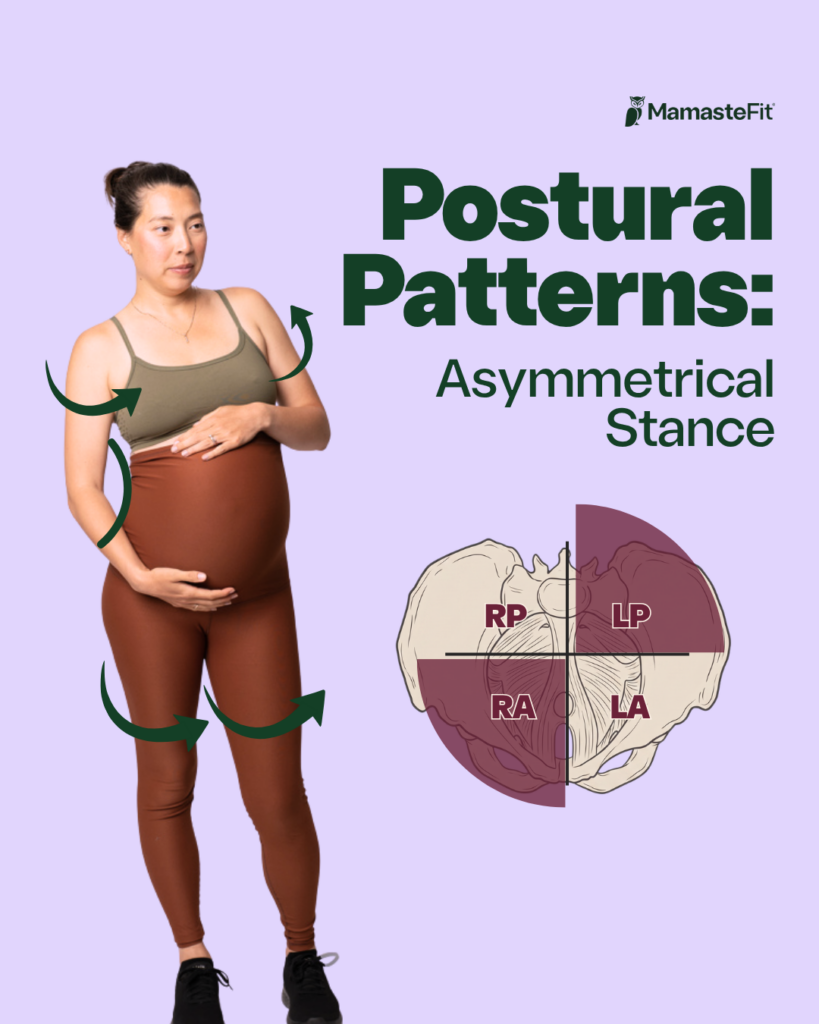
Support Your Pelvic Floor: Positioning with Asymmetry
Now let’s talk about the actual approach we use to return to running and sport after birth.
Before we can really dive into the running portion, we need to understand the foundation. One of the biggest mistakes I see is jumping straight into pelvic floor exercises without first understanding how the pelvis, rib cage, diaphragm, and pelvic floor all work together. When we understand the normal asymmetries throughout the body, we can make better decisions about which exercises actually support pelvic floor function.
This is one of the reasons our approach looks a little different than what you may have seen elsewhere. Rather than automatically prescribing clamshells, glute bridges, kegels, and generic core exercises, we want to understand how your body is managing pressure and movement. By supporting pelvic balance, we can create a better foundation not only for running but also for lifting, jumping, and returning to the activities you enjoy.
Pelvic Floor Asymmetry and Why It Matters
At MamasteFit, we don’t view the pelvic floor as a perfectly symmetrical structure. Instead, we recognize that the entire body is asymmetrical, and those asymmetries influence how pressure is distributed throughout the pelvis.
As a refresher, our common pattern tends to involve increased activity and tension within the right anterior and left posterior portions of the pelvic floor. The left anterior and right posterior portions tend to be relatively longer. This pattern aligns with common pelvic positioning, where the right hip tends to rest in a more tucked, internally rotated position, while the left hip tends to sit in a more extended, externally rotated position.
This asymmetrical positioning creates torque throughout the pelvis and pelvic floor. As pressure moves through the system during breathing, lifting, running, coughing, or daily movement, the pelvic floor must respond to those pressure changes. When one area consistently carries more tension and another consistently carries more length, the pressure may not be distributed as efficiently.
This does not mean asymmetry is bad. Every human body is asymmetrical. However, if someone is experiencing prolapse symptoms, supporting more balanced movement patterns throughout the pelvis may help improve symptom management and overall function.
Thoracic Asymmetry Influences Pelvic Floor Function
The pelvis is not the only area that demonstrates asymmetrical movement patterns. The rib cage and diaphragm also have predictable asymmetries that influence how pressure is distributed throughout the body.
Many spend a significant amount of time in extension with the rib cage elevated and reduced expansion through the backside of the body. In addition, we commonly see increased compression through the right anterior chest wall and reduced expansion through the left posterior thorax.
These asymmetries matter because the diaphragm is one of the primary structures responsible for managing pressure. If the rib cage cannot move effectively, pressure may not be distributed evenly throughout the abdominal cavity. Since the pelvic floor sits at the bottom of that pressure system, it often feels the consequences.
When we improve thoracic mobility and rib cage movement, we frequently see improvements in pressure management and prolapse symptoms. This is why many of our prolapse-focused programs begin with the rib cage and breathing mechanics rather than immediately focusing on the pelvic floor itself.
In this pelvic floor relaxation workout, I walk you through releasing common areas of tension in the thoracic spine and pelvis!
If you’re enjoying this deep dive into pelvic floor function, make sure you subscribe to our YouTube channel. We share free videos every week covering pelvic floor health, pregnancy fitness, postpartum recovery, birth preparation, strength training, and running.
Thoracic Mobility Exercises
The thoracic spine moves in all three planes of motion, which means improving thoracic mobility requires more than simply stretching your chest or doing a few cat-cows. To support pressure management and pelvic floor function, we want to improve the rib cage’s ability to move in the sagittal (front-to-back), frontal (side-to-side), and transverse (rotational) planes.
When working on thoracic mobility, I like to focus on three primary movement categories:
- Front-to-back thoracic mobility focuses on improving your ability to move between extension and flexion. One of my favorite options is a cat-cow variation with a strong emphasis on the back expansion portion of the movement. Many of us spend a significant amount of time in extension, so learning to create space at the back of the rib cage can be incredibly beneficial for pressure management.
- Side-body opening focuses on improving frontal-plane mobility. Because we often see greater tension on the right side of the body, I often emphasize movements that promote expansion and length in the right lateral rib cage and trunk. Side bends, side body openers, and breathing drills that encourage expansion of the right chest wall can all be helpful.
- Rotational mobility focuses on improving your ability to rotate through the thoracic spine. Rotation is an important part of walking, running, lifting, and everyday movement. I often emphasize left-sided rotational movements and left-side body crunch variations because they help improve your ability to move out of common asymmetrical patterns while also supporting left posterior expansion.

Our Pelvic Balance Approach
Now that we’ve addressed the thoracic component, let’s talk about the pelvis.
By understanding the normal asymmetries that exist within the pelvis and pelvic floor, you can use exercise to support better pelvic balance by releasing areas that tend to carry more tension and strengthening areas that tend to be more lengthened. Rather than randomly selecting stretches or strengthening exercises, this approach allows you to be more intentional with your movement and better support pelvic floor function.
We break down pelvic balancing in much greater detail in our Pelvic Balance blog, but below is an overview of the pelvic balance approach that we incorporate into all of our fitness programs. Whether you’re dealing with prolapse, leaking, pelvic pain, or simply looking to improve your body’s ability to manage pressure during exercise, these principles can be incredibly helpful.
Pelvic Balance: Stretching and Mobility Exercises
Your entire pelvic floor is not tight, nor is your entire pelvic floor loose. There is asymmetry in pelvic floor tension that we can consider when doing our stretches and mobility exercises.
For the right anterior pelvic floor, we often focus on groin and inner-thigh stretches and mobility exercises. These exercises help offload the anterior pelvic floor, which pulls the right pelvic half into internal rotation with adduction and a posterior position to support its movement, thereby allowing the right posterior pelvic floor to shorten.
For the left posterior pelvic floor, we frequently use hip shifts to release the deep gluteal muscles and posterior pelvic floor. Hip shifts help release the posterior pelvic floor, which pulls the left pelvic half into extension, external rotation, and abduction. Hip shifts are an exaggerated way that our pelvis moves as we come into stance while walking and running, so learning how to properly hip shift translates well to our return to running. We include a large variety of hip shifts within our fitness programs to support posterior pelvic floor release and pelvic balance.
One of the most important concepts is learning how to move between positions. The ability to transition from internal rotation to external rotation is often more valuable than trying to stay in one “perfect” position.
This is why we frequently use pelvic mobility exercises such as hip shifts, foam-roller hip shifts, 90/90 transitions, rotational lunges, and hip airplanes. These movements improve pelvic mobility while simultaneously teaching the pelvic floor how to respond to changing demands.
If you’d like a step-by-step progression rather than piecing together exercises from social media, our Postpartum Fitness Program includes guided pelvic balance workouts, mobility sessions, strength training, and return-to-impact progressions designed specifically for postpartum athletes.
Pelvic Balance: Strengthening Exercises
Stretching and mobility create opportunities for the pelvis and pelvic floor to change position, but strengthening exercises are what allow you to maintain and use those positions in daily life, during exercise, and while running. If mobility gives you access to a new position, strength helps you own that position.
In the upper body, we want to improve thoracic rotation, side bending, and the ability to move into a rounded or expanded back position. These movements help improve pressure distribution throughout the trunk and pelvic floor while also supporting the natural rotational mechanics that occur during walking and running.
One of my favorite exercises for this is the archer row. The archer row incorporates thoracic rotation, side bending, and back expansion while strengthening the upper back, obliques, and trunk. As you become more comfortable with the movement, it can be progressed to include a hip shift and pelvic rotation, allowing you to coordinate movement between the rib cage and pelvis. This exaggerated pattern helps reinforce the rotational mechanics that naturally occur during walking and running and can be a great way to improve overall movement quality while supporting pelvic floor function.
In the lower body, our approach varies depending on which portion of the pelvic floor we aim to support. On the right side, we often focus on strengthening the right posterior pelvic floor to help create better balance within the pelvis. Because the right hip commonly rests in a more internally rotated position, we want to incorporate exercises that improve our ability to access and control external rotation.
To do this, we typically utilize glute- and quad-dominant exercises such as squats, split squats, step-ups, and lunges that allow for a more upright torso position. We often pair these movements with an ipsilateral (same-side) hold and either abduction against a band or pressure into a foam roller. These strategies help bias the hip toward external rotation while encouraging greater activation of the musculature that supports the right posterior pelvic floor.
On the left side, we often focus on strengthening the anterior pelvic floor to improve balance throughout the pelvis. Because the left hip commonly rests in a more externally rotated position, we want to improve our ability to access and control internal rotation while strengthening the musculature that supports the anterior pelvic floor.
To do this, we typically utilize hamstring- and adductor-focused exercises, such as hinges, staggered-stance Romanian deadlifts, and other hip-dominant movement patterns. We often pair these movements with a contralateral (opposite-side) hold to bias internal rotation and to activate adduction by pressing into a long band, foam roller, or other object with the inner thigh or knee.
These strategies help improve the pelvis’s ability to move into and control internal rotation while strengthening the muscles that support the left anterior pelvic floor. Just as with the right side, the goal isn’t to force the pelvis into a perfect position. The goal is to improve your ability to access different positions and create greater balance throughout the system, so the pelvic floor can respond better to changes in pressure during lifting, running, and everyday movement.
If you’d like to see what this looks like in practice, check out our 30-Minute Pelvic Floor Balance Workout. In this workout, I walk you through mobility and strengthening exercises that target all four quadrants of the pelvic floor while incorporating the pelvic balance principles we’ve discussed throughout this article.
Whether you’re dealing with prolapse symptoms, leaking, pelvic pain, or simply looking to improve pelvic floor function, this workout is a great way to experience how mobility, strength, breathing, and pressure management can all work together to support the pelvic floor.
Quick Recap:
- Right Pelvis = Posterior Pelvic Tilt with Internal Rotation and Adduction
- This causes the right anterior pelvic floor to shorten, as the right posterior lengthens.
- Helpful approaches are the release with groin and adductor stretches and strengthening with quad/glute exercises that emphasize abduction and external rotation.
- Left Pelvis = Anterior Pelvic Tilt with External Rotation and Abduction
- This causes the left posterior pelvic floor to shorten, as the left anterior lengthens.
- Helpful approaches are to release the deep glute with hip shifts and strengthening with hamstring/adductor exercises that emphasize adduction and internal rotation.
Will I Have to Do Pelvic Floor Rehab Forever?
At this point, you may be thinking, “Great, now I have a list of exercises I’ll need to do forever.”
The good news is that the asymmetrical patterns we discussed are not unique to pregnancy, postpartum recovery, or prolapse. These are normal human movement patterns that exist in nearly everyone. Learning how to improve thoracic mobility, pelvic mobility, and pelvic floor balance can benefit anyone, regardless of whether they have a prolapse diagnosis.
That said, if you are experiencing prolapse symptoms, these movement strategies can be especially valuable. Supporting pelvic balance and improving pressure management often helps reduce symptoms while also improving overall movement quality.
The Missing Piece: Breath and Movement Coordination
Once we have improved thoracic mobility, pelvic mobility, and pelvic floor balance, the next step is learning how to coordinate breathing with movement.
Breath coordination is one of the most important aspects of pressure management. Every activity we perform creates pressure within the abdominal cavity. The amount of pressure generated depends on the demands of the task. Sitting on the couch requires very little intra-abdominal pressure, while lifting a near-maximal load requires significantly more.
This is not a bad thing. Intra-abdominal pressure is one of the body’s natural stabilization strategies. It helps support and protect the spine during movement.
When we inhale, the diaphragm descends and pressure within the abdominal cavity increases. When we exhale, the diaphragm ascends and pressure shifts upward. Depending on the demands of the task, we can simply allow the system to recoil and relax, or we can coordinate muscular activation during the exhale to better manage higher loads.
For many postpartum women, one of the easiest strategies is to inhale during the lowering portion of an exercise, exhale to prepare the pelvic floor, and then perform the harder portion of the movement. As strength increases, more advanced pressure management strategies become appropriate.
The goal is not to avoid pressure. The goal is to learn how to manage pressure.
If you’re still rebuilding your foundation postpartum, our Postpartum Fitness Program was designed specifically for this stage of recovery. We focus on improving strength, pressure management, mobility, and confidence before progressing into higher-impact activities.
Returning to Running With Prolapse
How Do You Know If You’re Ready to Start Running?
One of the most common questions we receive is, “How do I know if I’m ready to start running again?”
A commonly used return-to-running assessment includes being able to walk for 30 minutes, jog in place for one minute, balance on one leg, perform a single-leg squat, and hop on one leg. Ideally, you can complete these activities without significant compensation, pain, heaviness, pressure, leaking, or other prolapse symptoms.
However, it is important to remember that these assessments are simply tools. They are not pass-or-fail tests that automatically determine whether you can or cannot run. If you notice symptoms or struggle with one of these movements, it doesn’t necessarily mean running is off limits. Instead, it provides information about areas that may benefit from additional preparation.
Walking is often one of the best places to start. Building the ability to comfortably walk for longer durations helps develop endurance and prepares the body for the demands of running without the same level of impact.
What If Jogging in Place Doesn’t Feel Good?
Jogging in place can provide insight into how well you are managing impact and transferring weight from one leg to the other. However, jogging in place is not the same thing as running.
Many women find that stationary hopping or jogging feels more symptomatic than actual running mechanics. If you notice heaviness, pressure, or discomfort during these assessments, pay attention to your posture and positioning before assuming you are not ready.
One of the first things I look at is rib cage position. Can you bring the rib cage into a more neutral position instead of flaring upward? Can you find a little more arm swing and rotation through the trunk? Sometimes these simple adjustments can dramatically reduce symptoms almost immediately by improving how pressure is distributed throughout the body.
Preparing for Running
Before returning to running postpartum, we typically focus on several key foundations:
- Lower body strength
- Single-leg strength and stability
- Introductory impact exercises and plyometrics
- Walking or low impact cardio
Why We Start With Run-Walk Intervals
One of the biggest mistakes runners make after a long break is assuming they need to jump right back into continuous running.
Instead of starting with a three-mile or five-mile run, we typically begin with a run-walk-run approach. This may involve running for 30 seconds to one minute, followed by a longer walking interval before repeating the cycle for 15-30 minutes total at first.
This approach allows you to accumulate aerobic training while giving the pelvic floor, joints, muscles, and connective tissues opportunities to recover between impact-related bouts. It is one of the most effective strategies for returning to running after prolapse, pregnancy, or any extended break from training.
This is exactly what Roxanne used while preparing for her recent postpartum 10K. By using a run-walk progression, she completed the entire 6.2 miles without experiencing prolapse symptoms.
It’s also the same approach I used after my first baby. What started as stroller walks and short-run intervals eventually progressed to racing again, training for longer distances, and ultimately completing a sub-4-hour marathon postpartum.
If you’d like a structured progression rather than guessing your way through the process, our Return to Running Program walks you through exactly how we progress from walking to running while supporting the pelvic floor every step of the way.
If you’re more than 6 months postpartum and looking for a general strength-training program but also want to get back into running, our Beyond Postpartum Program includes a Beginner Running Program as well!
What My Running Looks Like Today
Today, my running looks very different from what it did at a year postpartum.
I typically complete one interval workout each week focused on shorter distances at faster paces. I also complete one tempo or threshold workout. In addition, I complete one long run each week lasting approximately 60 to 120 minutes.
These three workouts are my highest-priority running sessions. Any additional easy runs I complete throughout the week depend on my energy levels, recovery, and schedule. I also aim for 2-3 strength workouts per week!
Today, most of my training follows our Beyond Postpartum programming. Once you’ve rebuilt your foundation, the goal shifts from rehabilitation back toward performance, strength, endurance, and long-term fitness. If you’re ready to move beyond basic postpartum recovery and pursue bigger fitness goals, you can try Beyond Postpartum free for 7 days.
Can Running Make Prolapse Worse?
This is probably one of the most common questions women ask after receiving a prolapse diagnosis, and unfortunately there isn’t a simple yes or no answer.
Running does increase the demands placed on the pelvic floor. Every time your foot strikes the ground, force is transferred through the body and the pelvic floor has to respond to those changes in pressure and impact. However, that does not automatically mean running causes prolapse to worsen.
What we often see is that running can expose a capacity issue rather than create a problem. If the pelvic floor, surrounding muscles, and pressure management system are not yet prepared for the demands of running, symptoms such as heaviness, pressure, or leaking may appear. This does not necessarily mean damage is occurring. Instead, it may simply be a sign that your body would benefit from additional preparation, modifications to your training, or a temporary reduction in volume or intensity.
Think about it this way: if you tried to squat 300 pounds tomorrow and your legs gave out, we wouldn’t assume squatting is bad for you. We’d recognize that your current capacity doesn’t yet match the demand. Running after childbirth can be viewed through a similar lens. The goal is not to avoid running forever. The goal is to gradually build the strength, endurance, mobility, and pressure management strategies necessary to tolerate running comfortably.
This is one reason we spend so much time focusing on thoracic mobility, pelvic balance, strength training, breath coordination, and progressive return-to-impact work before increasing running volume. By improving your body’s ability to manage pressure and absorb force, we can often improve running tolerance and reduce symptoms.
It’s also important to remember that symptoms are only one piece of the picture. Research has shown that prolapse symptoms do not always correlate well with prolapse stage, meaning someone with more significant prolapse on examination may have very few symptoms, while someone with less prolapse may feel more symptomatic. Rather than focusing solely on the diagnosis itself, we encourage women to pay attention to how they feel, how they function, and whether symptoms are improving, staying the same, or worsening over time.
For many women, running becomes more comfortable as they continue rebuilding strength and capacity. In fact, both Roxanne and I have found that our ability to tolerate running has improved as we’ve continued strength training, improved our pressure management strategies, and gradually progressed our training loads.
The goal isn’t to avoid challenging your body. The goal is to challenge it appropriately so it can adapt.
If you’re currently experiencing heaviness, pressure, or leaking during your runs, check out our video on running modifications for prolapse symptoms. Sometimes small adjustments in posture, rib cage positioning, arm swing, or training structure can make a surprisingly big difference.
And if you’re not quite sure where to start, our Return to Running Program takes the guesswork out of rebuilding after childbirth by walking you through the exact progression we use with our postpartum athletes.
What If You Experience Symptoms While Running?
Experiencing symptoms during a run does not automatically mean you should stop running forever.
Instead, view symptoms as information.
If you notice heaviness, pressure, or leaking during a run, first consider whether positioning adjustments might help. Improving thoracic mobility, finding a more balanced rib cage position, and improving rotational movement through the trunk can often reduce symptoms surprisingly quickly.
You may also benefit from temporarily increasing the amount of walking within your run. Returning to shorter run intervals often allows you to continue building aerobic fitness while reducing symptom irritation.
Remember that symptom fluctuations are normal. A symptomatic run does not necessarily mean your prolapse has worsened.
A Prolapse Diagnosis Does Not Mean Your Active Life Is Over
Returning to running after childbirth can feel intimidating, especially if you have received a prolapse diagnosis. Unfortunately, many women are told that they should never run again, never lift weights again, or avoid exercise altogether.
That message is not only discouraging, but it also ignores the tremendous benefits of movement.
Exercise is one of the most powerful tools we have for supporting physical and mental health. Strength training becomes increasingly important as women age. Cardiovascular exercise supports heart health, endurance, and overall quality of life. Movement helps us feel capable in our bodies.
A prolapse diagnosis may change how you approach training, especially in the early stages of recovery, but it does not automatically mean you need to stop pursuing the activities you love.
Last weekend, Roxanne crossed the finish line of her first postpartum 10K after her fourth baby. In October, we’ll be lining up together again for a 5K, 10K, and half marathon challenge weekend. Neither of us has a perfect pelvic floor. Both of us have prolapse. Both of us have experienced different postpartum recoveries.
What we do have is a willingness to keep learning, keep adapting, and keep pursuing goals that matter to us.
A prolapse diagnosis does not mean your active life is over. It simply means your journey may look a little different than you expected.
Ready to Get Started?
- Download our Free Pelvic Floor Exercise Guide
- Explore our Postpartum Fitness Program
- Check out our Return to Running Program
- Try Beyond Postpartum free for 7 days
- Subscribe to our YouTube channel for more free education, workouts, and pelvic floor resources
References:
- Broekhuis SR, Fütterer JJ, Hendriks JCM, et al. Symptoms of pelvic floor dysfunction are poorly correlated with findings on clinical examination and dynamic MR imaging of the pelvic floor. Int Urogynecol J. 2009;20(10):1169-1174.
- Dietz HP, Shek KL, Chantarasorn V, et al. Pelvic organ prolapse in nulliparae. Aust N Z J Obstet Gynaecol. 2022;62(3):403-408.
- Larsudd-Kåverud J, et al. The influence of pregnancy, parity, and mode of delivery on pelvic floor disorders. Am J Obstet Gynecol. 2023.