



Table of Contents
Birth Prep Exercises and Pelvic Mobility
During pregnancy, there is a lot of emphasis on birth preparation. You have nine months to prepare for birth, and part of that birth preparation is doing birth prep exercises to physically prepare your body for labor. You cannot control every aspect of your labor, but you can certainly set the conditions in your favor.
If we can improve pelvic mobility, balance tension within the pelvic floor, and ensure that you can change positions to create space in each part of the pelvis, this is going to make that aspect of labor easier. Labor will still be challenging! But we can surely set the conditions in our favor by improving how well you can create space within your pelvis and, in turn, help your baby move through the pelvis.
In this blog, I’m going to break down how you can create space in each of the pelvic levels and what movement patterns you need to be able to do to open the entirety of the pelvis, both with mobility exercises and strengthening exercises.
We need both mobility and strength because mobility helps to release tension to make the movement available to us, but we need strengthening exercises to actually pull the pelvis into different positions. A combination of both can really help support your birth preparation.
Opening the Pelvis
Before we can dive into what movements help create space in the pelvis, we need to better understand the different pelvic levels.
It is important to know is that your pelvis can move. It is not a solid bone that is immobile. There is movement capability at the pelvic joints.
Now, the pelvis does not have the same movement capability as your shoulder or your hip joint. The movement in the joints is fairly small, but even a few millimeters of movement can greatly impact pelvic diameters and influence tension within the pelvic floor.
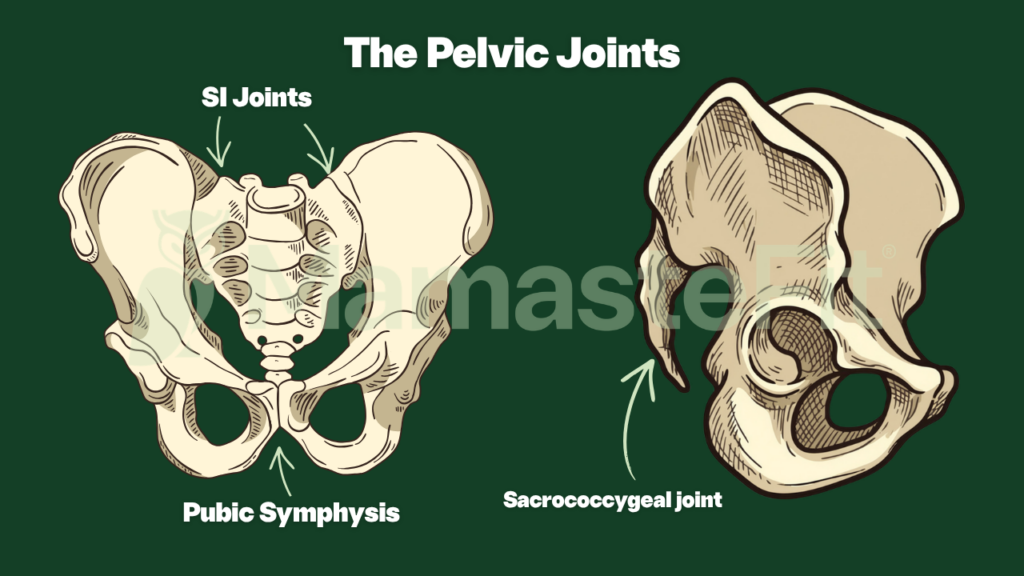
There are different components to your pelvis that allow it to open and change diameters. The pelvis has four joints: the pubic symphysis joint on the front, the sacroiliac joints on the back, and the sacrococcygeal joint at the tailbone. These four joints allow for displacement of the innominate bones and your sacrum.
During pregnancy, the movement and displacement of these pelvic joints increases thanks to hormonal changes, including relaxin, increased estrogen promoting connective tissue hydration and collagen remodeling, progesterone increasing smooth muscle relaxation and reducing muscular tone, and prostaglandins during labor supporting connective tissue remodeling, cervical ripening, and soft tissue flexibility. These hormonal changes help the ligaments and connective tissues surrounding the pelvis become more compliant and adaptable, allowing for greater movement capability within the pelvic joints during pregnancy and labor.
Understanding how the pelvis moves is one thing, but actually being able to access these movement patterns is another. This is why our prenatal fitness programs include pelvic mobility, strengthening, and birth preparation movements in every workout. We combine mobility work to make movement available with strengthening exercises to help you actively move and control your pelvis throughout pregnancy and labor preparation.
Whether you prefer self-paced app-based workouts or follow-along video workouts, our prenatal programs are designed to help you feel stronger, more comfortable, and more prepared for birth.
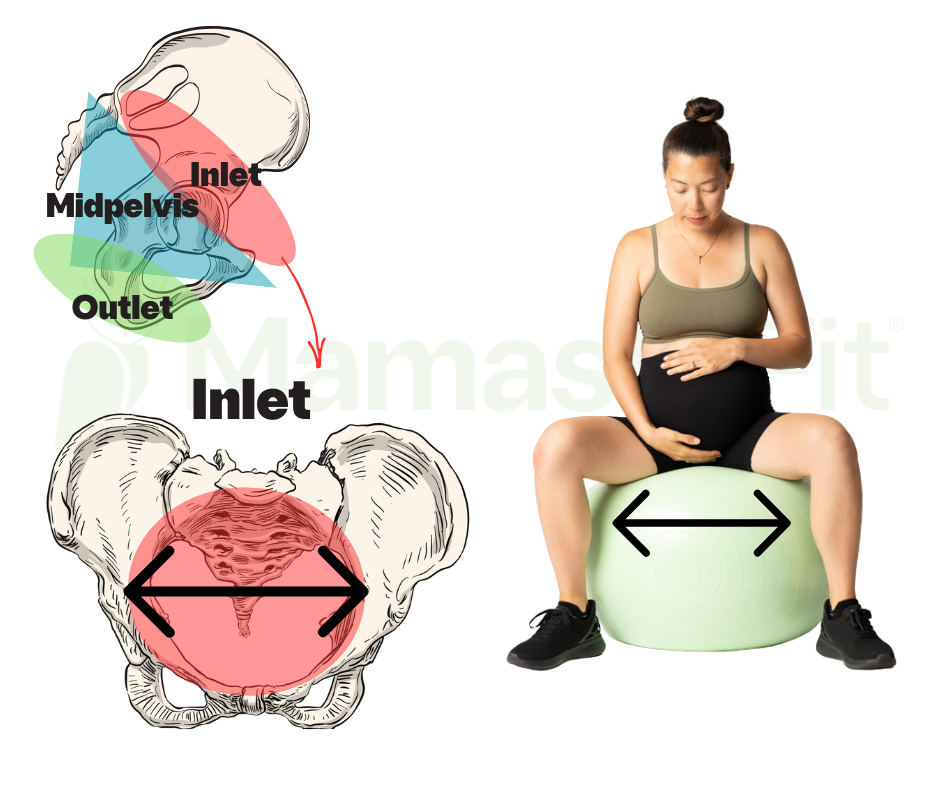
The Pelvic Inlet: Creating Space at the Top of the Pelvis
The top of the pelvis is the pelvic inlet, and this is where the baby will first enter or engage into the pelvis.
The pelvic inlet is defined by several pelvic diameters, including the anterior-posterior diameter, also known as the obstetric conjugate, the transverse diameter, and the oblique diameters. The anterior-posterior diameter runs from the sacral promontory toward the pubic symphysis, the transverse diameter measures the side-to-side width across the inlet, and the oblique diameters run diagonally across the pelvis. The transverse diameter is generally the widest portion of the pelvic inlet, which is one reason babies commonly engage into the pelvis in an occiput transverse or slightly oblique position.
The movement patterns that help create space in the top of the pelvis include external rotation with abduction in the pelvis and anterior and posterior pelvic tilt. We expand on pelvic inlet opening by also incorporating the anterior pelvis, which I normally find to be excluded from the conversation around how to create space in the top of the pelvis.
External rotation with abduction in the pelvis creates more opening side to side in the top of the pelvis. Emphasizing positions that involve wider knees, such as deep squats, butterfly pose, and straddle pose—typically very common birth prep exercises—can help prepare you to create space in the top of the pelvis.
Note on Pelvic Pain with Inlet Opening
Now, if you have pelvic pain, especially pubic symphysis pain or SPD, you may find that wide-leg positions are painful and inaccessible.
It is important during pregnancy that we address pelvic pain because this can be a sign that pelvic mobility is limited, which may or may not have an impact on birth. But I will say that very small movements during labor can still be very impactful.
So if you cannot find a super deep squat with really wide-leg positions because it is painful, you will probably be fine during labor because you do not need huge movements to support your baby’s rotation through the pelvis.
In addition, as baby enters into the pelvis, this internal pressure change can help provide some pelvic stability and you may find that you do not even notice your SPD.
With that, it is still important that we address pelvic mobility because it can, one, help keep you more comfortable throughout your pregnancy and, two, likely positively impact your labor.
If you are dealing with pelvic pain, know that you do not have to simply push through it or avoid movement altogether.
Our prenatal fitness programs include pelvic mobility and stability work to help support common pregnancy discomforts while also preparing your body for labor. Many women find that when they improve how well their pelvis can move and stabilize, they feel more comfortable not only in workouts but also in daily life and birth preparation.
Pelvic Tilting and the Pelvic Inlet
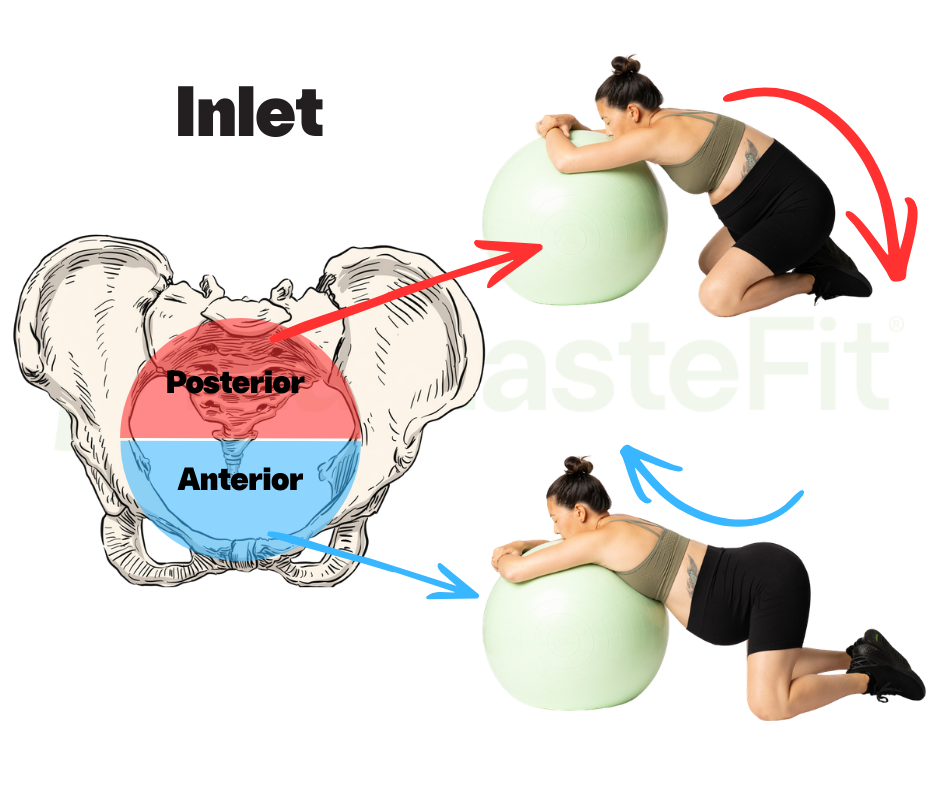
Now, the other aspect of creating space in the pelvic inlet is anterior and posterior pelvic tilting.
As I previously discussed, anterior pelvic tilt is typically excluded from the movement patterns required to create space in the top of the pelvis. Typically, you will only see a posterior pelvic tilt advertised as a pelvic inlet-opening movement.
A posterior pelvic tilt helps move the sacral promontory backward, which is the junction between the lumbar spine and the sacrum, and creates more space in the posterior inlet. This movement pattern is incredibly important and also sometimes more restricted during pregnancy, which we will discuss momentarily.
Anterior pelvic tilt, or arching more in the back, changes the pubic bone angle, creating more space in the anterior inlet. This can be incredibly helpful in helping baby get behind the pubic bone and then drop into the pelvis and is typically why several “magic moves” of labor, such as Walcher’s and Flying Cowgirl, tend to work so effectively in helping a baby engage.
Anterior pelvic tilt also helps make external rotation easier to achieve based on how pelvic position changes the orientation of the femur in the hip socket. When we have more of an anterior pelvic tilt, the hip joint tends to move forward, making external rotation easier.
Now, coming back to posterior pelvic tilt being more challenging.
During pregnancy, there are common postural tendencies that make it easier to achieve certain movement patterns and positions. We tend to favor more extension in the spine, which makes an anterior pelvic tilt typically easy to find, and we tend to favor more external rotation. So, two out of the three movements required to create space at the top of the pelvis are typically easier to find during pregnancy.
Being that a posterior pelvic tilt is also incredibly important, this becomes a major emphasis in our birth prep programming to help you find a more rounded-back position and support better pelvic mobility.
In our birth preparation circuit, we incorporate three movements that help you find more of a posterior pelvic tilt because of how important it is to support labor progress.
Baby Struggling to Engage?? Try this.
If your baby is struggling to engage—which does not need to happen until labor—sometimes focusing on exercises that help increase your ability to find a rounded back and tuck your pelvis underneath can help baby drop into the pelvis.
You can explore this YouTube video here, which explains different movements that you can do prenatally and during labor to help baby engage.
Be sure to subscribe to our YouTube channel for more than just free workouts.
We share weekly education and movement videos covering birth preparation, pelvic mobility, labor positioning, pelvic floor function, pregnancy discomfort relief, postpartum recovery, and strength training throughout motherhood. Our goal is to help you better understand why movement matters and give you practical ways to apply it throughout pregnancy, birth, and postpartum.
And if you want more support than free videos alone, our prenatal fitness programs take this education further with structured workouts that incorporate pelvic mobility, birth preparation movements, and pregnancy-specific strength training into every week of programming. We offer both self-paced app-based programming and follow-along video workouts depending on how you prefer to train.
The Midpelvis: Rotation and Diagonal Space
The next level of the pelvis is the midpelvis.
The middle of the pelvis opens more with diagonal movement in the pelvic diameters. The primary diameter of the midpelvis is the interspinous diameter, sometimes referred to as the bispinous diameter, which is the distance between the ischial spines and is often considered the narrowest portion of the pelvis. There are also anterior-posterior and sagittal dimensions that contribute to the available space in the midpelvis. The interspinous diameter is particularly important because this is often where rotation and descent become more mechanically challenging for baby.
The middle of the pelvis opens more with asymmetrical movements and weight shifting from side to side.
Movement patterns that emphasize one-sided external rotation with abduction and anterior pelvic tilt, along with one-sided internal rotation with adduction and a posterior pelvic tilt, help create space in different parts of the midpelvis.
We can subdivide the midpelvis into two levels: the upper midpelvis and lower midpelvis.
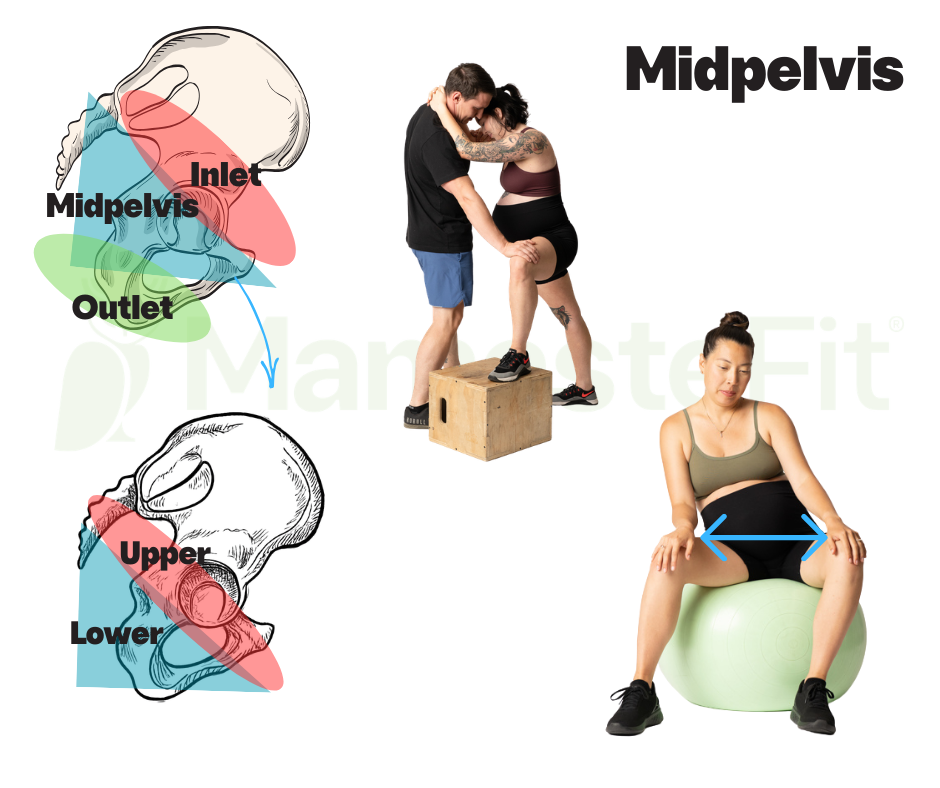
The upper midpelvis is where the baby first enters and begins to rotate through the pelvis. The upper midpelvis is going to open more with open-hip positions and typically a non-stance or unloaded leg. This can include more external rotation and abduction with an anterior pelvic tilt and movements such as an elevated lunge or movements where the leg is moving away from midline.
The lower midpelvis is where the baby finishes the rotation underneath the pubic bone.
This area of the pelvis may have more restrictions, similarly to that posterior pelvic tilt, based on those common postural tendencies.
The lower midpelvis opens more with internal rotation and adduction with a slight posterior pelvic tilt, typically in the stance or loaded leg. This is going to look more like the pelvis rotating more toward the femur in closed-hip or hip-shifted positions.
Being that this type of movement pattern can be more challenging for somebody during pregnancy, it should be a big emphasis in a prenatal or birth preparation program.
When we cannot find internal rotation in the pelvis, this can create more late labor stalls where baby has a hard time finishing the rotation out of the pelvis. This can be known as a deep transverse arrest, a late labor stall, or even cause prolonged pushing where baby seems to be struggling to get underneath the pubic bone.
We can incorporate exercises that involve increased pelvic mobility where we find both internal and external pelvic rotation to help improve how well baby can navigate through the midpelvis.
It is important to note that pelvic mobility is different than hip mobility.
Pelvic mobility relates to how the pelvis moves on the femur, typically in closed-chain positions, while hip mobility is how the femur moves on the pelvis, typically in open-chain positions.
You can watch this YouTube video that breaks this down in more depth with some exercise examples.
This is one of the biggest differences in our prenatal programming.
Many exercise programs focus only on stretching or traditional hip mobility, but we incorporate both hip mobility and pelvic mobility into our prenatal workouts because they are not the same thing.
Every week inside our prenatal programs, we include movements that help you access internal and external pelvic rotation, improve pelvic mobility, and build the strength required to actually control these positions. Birth preparation is not just about being flexible—it is also about having access to movement and the strength to use it.
Whether you prefer self-paced app-based programming and follow-along video workouts, our prenatal programs are designed to support a strong, comfortable pregnancy while preparing your body for labor.
Midpelvis Exercises and Movement Patterns
In a birth preparation or prenatal program, we tend to incorporate a lot of hip-shifted exercises that emphasize internal rotation and adduction, both in mobility work with hip shifts and with strengthening exercises such as a staggered-stance RDL with banded abduction.
Because many pregnant women already tend to favor more extension and external rotation, these closed-hip and internally rotated positions can often be the missing piece in birth preparation.
This is one reason we place such a strong emphasis on unilateral work and pelvic rotation throughout pregnancy.
The Pelvic Outlet: Creating Space for Pushing
The bottom of the pelvis is known as the pelvic outlet. This area of the pelvis typically needs to be opened when you are pushing.
The pelvic outlet is defined primarily by the anterior-posterior diameter, the posterior sagittal diameter, and the transverse or intertuberous diameter between the ischial tuberosities. Unlike the pelvic inlet, where the transverse diameter is widest, the pelvic outlet has a wider anterior-posterior diameter and a narrower transverse dimension. This change in shape is one reason baby must rotate as they descend through the pelvis.
The pelvic outlet opens more with internal pelvic rotation, with adduction and a slight posterior pelvic tilt.
We differ in our recommendations to open the pelvic outlet from other pelvic mechanic-focused educators. Other educators tend to promote that an anterior pelvic tilt creates more space in the pelvic outlet, but we find an anterior pelvic tilt does not align as well with pressure management strategies and tends to not be very intuitive for our clients as they are pushing.
A posterior pelvic tilt makes internal rotation easier because it changes the orientation of the femur in the hip socket.
Other considerations for the pelvic outlet are that it is more soft tissue than bony architecture. The pelvic outlet is different than the inlet and midpelvis, which have more bony structure and where we need to influence pelvic diameters more. The pelvic outlet is mostly soft tissue, so finding positions that help somebody yield and relax is often more important than forcing the pelvis more open.
In addition, since pushing is a pressure management activity, finding a more neutral or slightly rounded position can help increase the strength of the pushes based on the diaphragmatic angle and its orientation to the pelvic floor.
I have very rarely seen someone intuitively find a more arched position while pushing. This typically only happens if someone’s baby is OP, where the back of their baby’s head is toward the back of the pelvis, based on how an OP baby needs to navigate underneath the pubic bone. But intuitively, most will find more neutral positions with their legs and a more stacked or rounded position with their upper body because of how this positively supports pressure management.
Another consideration for the pelvic outlet is that when baby is navigating the pelvic inlet and the midpelvis, only the baby’s head is navigating the pelvis at that time. Once baby has made it to the pelvic outlet, they have finished rotating underneath the pubic bone and their body is now also navigating the pelvis. So, a little bit of the conversation becomes: when we emphasize opening of the pelvic outlet, how might that impact baby’s body ability to navigate through the pelvis?
This is a newer conversation that we are having, but an important consideration when we think about birth preparation.
Here is our YouTube video where we break down some of our newer and different approaches to opening the pelvic outlet as a part of birth preparation.
Birth preparation is not just about opening your pelvis as wide as possible.
It is about understanding which movement patterns create space in different areas of the pelvis and having the strength, mobility, and coordination to access those positions when labor begins.
This is exactly why our prenatal programs include birth preparation circuits, pelvic mobility work, strengthening exercises, and labor-focused movement patterns throughout pregnancy. We help you train these movement patterns before labor so they feel more intuitive and accessible when you need them.
Birth Prep Movements: What Movements Do We Actually Need?
Now that we understand how to create space in each of the pelvic levels, let’s break down what movements we need to be able to access to help set the conditions in our favor for birth.
To create space in the pelvis, we need:
- Bilateral external rotation with abduction
- Unilateral external rotation with abduction
- Unilateral internal rotation with adduction
- Bilateral internal rotation with adduction
These movement patterns help us access different portions of the pelvis and support the positional changes required throughout labor. The goal is not to force baby into any specific position or to guarantee a particular birth outcome. Instead, the goal of birth preparation is to ensure that these movement options are accessible to us so that when labor begins, we can more easily change positions and create space throughout the pelvis.
1. Bilateral External Rotation With Abduction
Bilateral external rotation with abduction can look like movements such as a deep squat for mobility and a weighted squat for strengthening. These movements help create side-to-side space in the pelvis and are often some of the more intuitive movement patterns during pregnancy because of those common postural tendencies toward extension and external rotation.
That does not mean they are unimportant—quite the opposite.
These positions still play a major role in helping us create space at the pelvic inlet and improving pelvic mobility throughout pregnancy.

2. Unilateral External Rotation With Abduction
Unilateral external rotation with abduction can look like open-hip positions, such as the lateral hip shift for mobility, weighted lateral hip shifts for strengthening, and a B-stance squat with an ipsilateral hold.
All of these movements help target strengthening of the quadriceps and glute musculature while emphasizing external rotation and abduction. These exercises are particularly helpful for creating asymmetrical movement through the pelvis and supporting mobility within the upper midpelvis. Because labor is rarely perfectly symmetrical, having the ability to move and stabilize in asymmetrical positions can be incredibly valuable.

3. Unilateral Internal Rotation With Adduction
Internal rotation with adduction can look like closed-hip stance positions, such as the hip shift for mobility and a staggered-stance RDL with banded abduction and an ipsilateral hold for strengthening, with an emphasis on the hamstrings and inner thighs.
These movement patterns are often the missing piece during pregnancy because they can feel less intuitive. Many women naturally favor more extension and external rotation during pregnancy, making these internally rotated and more closed positions harder to access. But as we discussed in the midpelvis section, these movements are often incredibly important for helping baby complete rotation through the pelvis.
This is one reason we place so much emphasis on hip shifts, pelvic rotation, and unilateral strengthening within our birth preparation programming.

4: Bilateral Internal Rotation With Adduction
Bilateral internal rotation with adduction can look like back-expansion exercises with a block squeeze for mobility and hinge exercises with a block squeeze or a suitcase deadlift for strengthening.
These movement patterns help emphasize internal rotation and adduction while also encouraging more posterior expansion and helping us access those rounded positions that may otherwise be more challenging during pregnancy.
Again, the goal is not to live in one posture or chase perfect alignment. The goal is movement variability. The better we can access and move between different pelvic positions, the more movement options we have available to us during labor.

If this feels like a lot, know that you do not have to figure this out alone.
We have free YouTube workouts and birth preparation education that walk through many of these movement patterns, and our prenatal fitness programs take it a step further with structured workouts designed specifically for pregnancy. Every workout includes mobility, strength, and pelvic movement strategies to help you stay strong and comfortable while preparing for labor.
Conclusion: Birth Preparation Requires Variety
When it comes to birth preparation, there is no one best exercise because the pelvis is not one single opening and labor is not one single movement pattern. Different parts of the pelvis open with different positions and movement strategies, which means birth preparation should include a variety of movement patterns to help create space throughout the entire pelvis. The goal is not to force baby into position or guarantee a particular labor outcome. Birth is complex, and many factors influence how labor unfolds. But what we can do is help improve pelvic mobility, balance tension within the pelvic floor, and ensure that we can access a variety of movement options to support the normal movement patterns of labor.
Mobility helps make movement available, but strength helps us actually control and access those positions. This is why birth preparation cannot simply be stretching or mobility work alone. We need mobility to release tension and improve movement availability, but we also need strengthening exercises to help pull the pelvis into different positions and support stability as baby navigates through the pelvis. Together, mobility and strength help create a more adaptable and responsive body that is better able to change positions throughout labor and support the different movement demands required at the inlet, midpelvis, and outlet.
As we discussed throughout this blog, some movement patterns are often easier to find during pregnancy, while others may require more intentional practice and strengthening. Wider positions and external rotation may already feel accessible, while internally rotated, hip-shifted, or more rounded positions may feel more challenging. This does not mean one movement is better than another or that we should live in any one position. Rather, the goal is movement variability and ensuring that these different movement options are accessible to us when labor begins.
This is exactly why we approach birth preparation differently inside our prenatal fitness programs. Rather than focusing on one magic exercise or generic labor prep stretches, we incorporate pelvic mobility, strengthening, birth preparation movements, and labor-focused exercise progressions into every week of programming. Our workouts are designed to help you build strength, improve comfort, and better understand how your body moves so that you feel more prepared for pregnancy, labor, and beyond. Whether you prefer self-paced app-based programming and follow-along video workouts, we guide you through these movement patterns step-by-step so you can train with intention and confidence throughout pregnancy.
Frequently Asked Questions
Birth preparation can bring up a lot of questions, especially when social media often promotes one “best” position, one magic exercise, or rigid rules around pregnancy and labor. The reality is that birth is dynamic, and preparing for labor is often more nuanced than quick tips and simple answers. Below are some of the most common questions we get about birth preparation, pelvic mobility, and labor positioning.
What Is the Best Position for My Baby to Be in for Birth?
There is no one best position for birth.
Baby needs several positions and movement options throughout labor, and their position during pregnancy does not determine how your labor will go or when labor will start. Babies move and rotate throughout pregnancy and labor, and many babies do not begin labor in one perfect textbook position.
When people talk about the “best” position for birth, they are often referring to a baby who is head down, or vertex, with the back of their head toward the front of the pelvis. This is called occiput anterior, or OA. While OA may be a common position for birth, it is important to understand that labor is much more nuanced than labeling one position as good and another as bad.
Many babies engage into the pelvis in an occiput transverse or slightly diagonal position and rotate during labor. Others may begin labor more posterior, or sunny side up, and still rotate and be born vaginally. Babies are dynamic, and labor itself is often part of the rotational process.
Rather than trying to force baby into one perfect position during pregnancy, we tend to focus more on creating an environment where baby has movement options. This includes improving pelvic mobility, balancing tension within the pelvic floor, and ensuring that mom can comfortably access a variety of movement and labor positions. A pelvis that can move and change positions often gives baby more opportunity to navigate labor efficiently.
It is also important to remember that fetal positioning is only one piece of the labor puzzle. Baby size, pelvic shape, uterine contractions, soft tissue tension, labor positions, and many other factors can all influence how labor unfolds. Birth preparation is not about guaranteeing one specific baby position or birth outcome, but rather improving movement options and creating favorable conditions to support labor.
My Baby Is OP, Sunny Side Up, or Posterior—What Can I Do?
First, if your baby is posterior, try not to panic.
Posterior, sunny side up, or occiput posterior (OP) means that the back of baby’s head is toward the back of the pelvis rather than toward the front. Many people immediately hear that OP is a “bad” position, but it is important to know that babies can and do rotate during labor, and vaginal birth is still very possible with an OP baby.
Rather than viewing posterior positioning as something that always needs to be corrected, we prefer to think about how to create movement options and space within the pelvis.
As we discussed in the midpelvis section, rotation is a huge component of labor. The midpelvis opens more with asymmetrical movement and pelvic rotation, and this is often where babies need to complete significant rotational changes. Exercises and labor positions that emphasize pelvic mobility, weight shifting, asymmetrical movement, and both internal and external pelvic rotation may help improve how well baby can navigate the pelvis.
It is also important to understand that not all posterior babies are the same. Some babies may be temporarily posterior and rotate early in labor, while others may remain posterior longer and still rotate during pushing or be born posterior.
This is one reason we emphasize movement variability rather than rigid positioning rules. Movement can help create opportunities for rotation, but we cannot guarantee or force baby into one specific position.
You can explore our YouTube video here where we break down movement and labor position strategies for posterior babies and discuss why rotation through the midpelvis is often such an important part of the conversation.
My Baby Isn’t Engaged Yet—What Should I Do?
First, it is important to know that engagement does not need to happen until labor.
Many first-time moms may have babies engage earlier, sometimes weeks before labor begins, while subsequent pregnancies often engage much later or even during active labor. So if your baby is still high or “floating,” this does not automatically mean something is wrong.
When baby has not engaged, we often think about how to create more space at the pelvic inlet. As we discussed earlier in this blog, the pelvic inlet opens with external rotation and abduction along with both anterior and posterior pelvic tilting. Many women naturally already have access to wider positions and anterior pelvic tilt during pregnancy, but may have a harder time accessing posterior pelvic tilt or more rounded positions.
Sometimes helping baby engage can involve improving mobility and access to those posterior pelvic tilt positions, encouraging movement variability, and practicing exercises that help baby move behind the pubic bone and descend into the pelvis. Movements such as posterior pelvic tilting, rounded positions, and certain asymmetrical labor positions may be helpful.
That said, it is important to remember that a baby not being engaged before labor is not necessarily a problem to fix. Labor itself creates contractions, pressure changes, and movement within the pelvis that often support engagement naturally.
You can explore this YouTube video here where we break down movement strategies that may help support engagement during pregnancy and labor.
When Can I Start Birth Prep Exercises?
Really, anytime.
You do not need to wait until your third trimester to start birth prep exercises. Movement does not put you into labor, so doing birth prep exercises will not induce labor. Rather than thinking about birth preparation as something that only matters at the very end of pregnancy, we tend to think about it as improving movement options and preparing your body throughout pregnancy.
How early you start may also depend on your individual movement capability. If you have more restrictions in your pelvic mobility, hip mobility, or movement patterns, you may need more time to improve those mechanics compared to someone who already has greater movement availability. This is one reason we encourage birth preparation throughout pregnancy rather than waiting until the last few weeks. Birth prep is not about rushing to force changes at the end of pregnancy, but gradually improving movement variability, mobility, and strength over time.
How Often Should I Do Birth Prep Exercises?
You can absolutely do birth prep exercises daily, but how you incorporate them will vary depending on your workout preferences and your available time.
At a minimum, you could do our birth prep circuit a few times per week, which we program as the warm-up to our prenatal workouts. Or, you could complete one of our prenatal workouts three to four times per week, which includes birth prep exercises within every single workout.
It is also important to understand that exercises do not need to be labeled specifically as “birth prep” to support labor preparation. As we discussed throughout this blog, the goal is to access the four movement patterns that create space throughout the pelvis. If your workouts are already emphasizing bilateral external rotation with abduction, unilateral external rotation with abduction, unilateral internal rotation with adduction, and bilateral internal rotation with adduction, then you are already incorporating movement strategies that may support birth preparation.
Birth prep is often less about adding more exercises and more about being intentional with the movements you are already doing.
Do I Need to Keep Perfect Posture for Optimal Positioning and an Easier Labor?
No.
There is no one perfect position that you need to maintain throughout pregnancy, and honestly, this rhetoric often increases anxiety and tension more than it helps. The best position is usually the next one.
We want the ability to change positions rather than maintain static upright positions all the time. Your baby is not going to become “stuck” because you sat on the couch or relaxed in one position for part of the day. Pregnancy and birth are dynamic, and your body is designed to move and adapt.
With that said, if you find yourself in the exact same position all the time, then this may influence pelvic mobility and tension balance. The concern is usually not one individual position but rather a lack of movement variability.
This is why we place such a large emphasis on movement options and position changes during pregnancy rather than chasing perfect posture or ideal alignment. The goal is not to hold yourself in one specific posture, but to improve your ability to comfortably move between different positions and access different movement strategies when you need them.