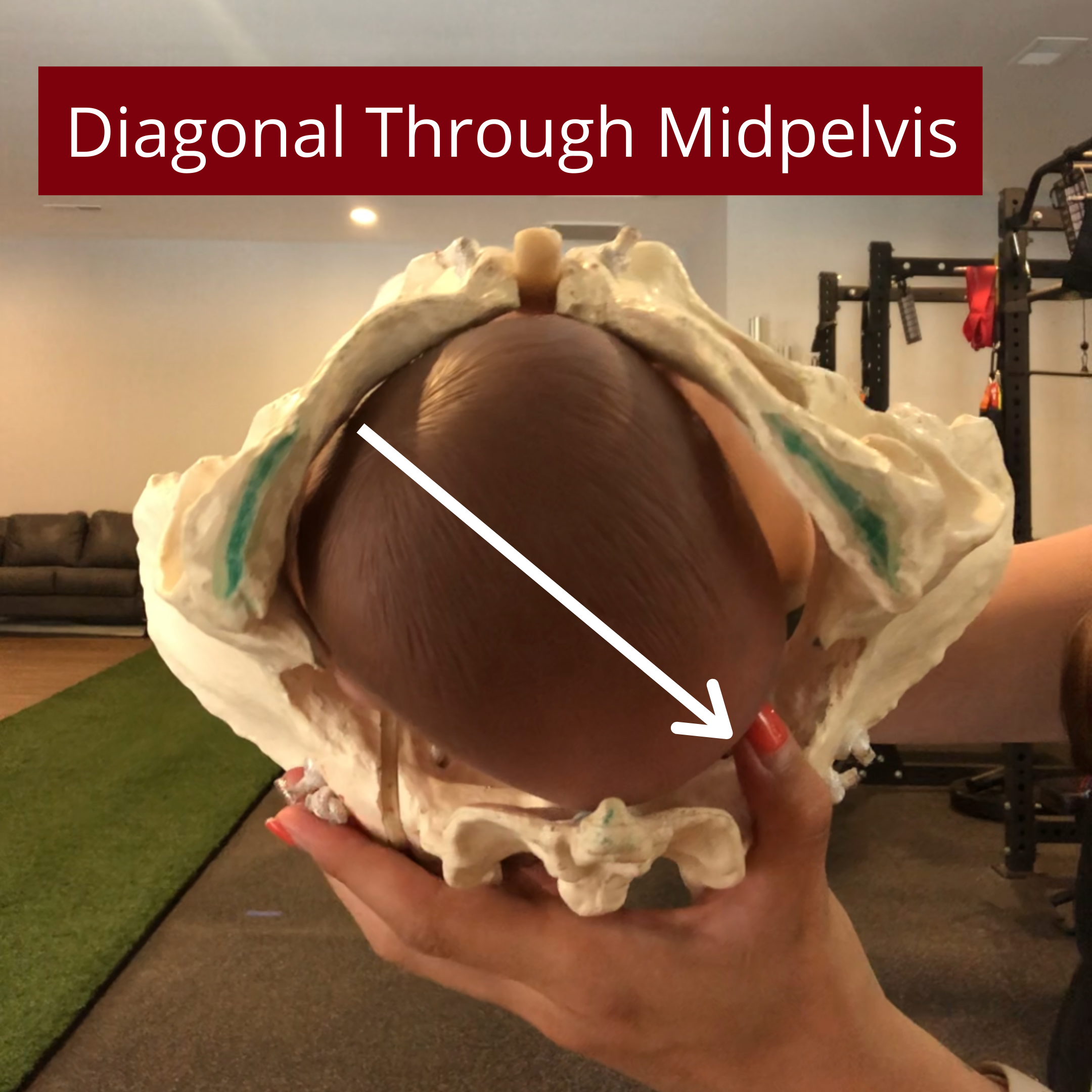


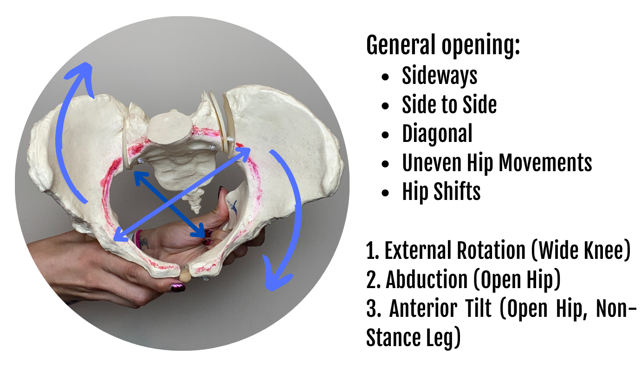
The midpelvis opens with asymmetrical movement patterns: one hip is doing something differently than the other. This creates more space diagonally, allowing baby to better fit through this pelvic level. But, we may want to emphasize certain movement patterns based on where baby is in its rotation through the midpelvis. If baby is beginning their rotation, we may want to create more space in the upper midpelvis. This may be -1 to 0 station.
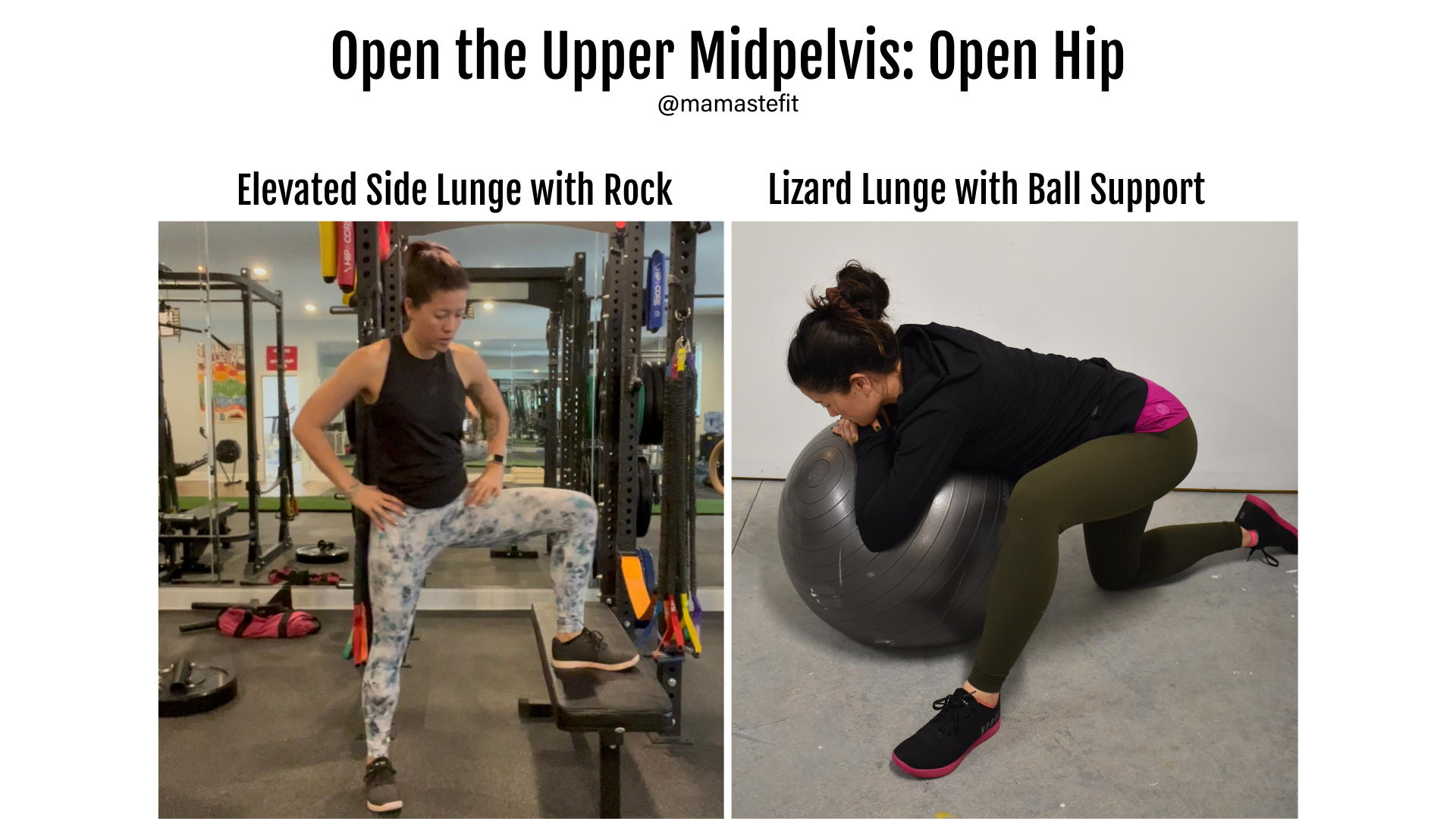
We can open the upper midpelvis more with external rotation of the femur (open hip, or wide knee) on the side baby is on (most likely left), abduction (leg moving outwards), and an anterior pelvic tilt (pelvis falling forward on that side). How can we achieve this? Focus on an open hip position, where the angle at the femur and hip crease is greater than 90 degrees. You can also think drive the knee forward, and this tends to open the hip angle, as well!
You could try movements such as: elevated side lunge with rocking or lizard lunge with ball support!