



Table of Contents
If you’re preparing for birth, one of the topics that often comes up — but isn’t always fully explained — is fetal monitoring. How will your baby be monitored during labor? What do the different methods mean? And most importantly, what choices do you actually have?
In this blog, we’re breaking down everything you need to know about fetal monitoring: what it is, how it works, the differences between continuous fetal monitoring and intermittent auscultation, the evidence behind both approaches, and how you can use this information to advocate for the type of care that feels right for you.
Subscribe to our YouTube Channel for more weekly workouts and educational videos! We publish one new workout video and 2-3 educational videos a week on our channel.
What Is Fetal Monitoring?
Fetal monitoring is the process of tracking your baby’s heart rate and your contraction pattern during labor to assess how well your baby is tolerating labor.
With monitoring, providers evaluate two main things:
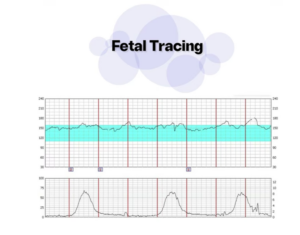
Baby’s heart rate
Your contraction pattern
When these are tracked together, they create a tracing that helps providers assess fetal well-being and determine whether baby is thriving, needs closer observation, or needs immediate intervention.

Why Was Continuous Fetal Monitoring Created?
Continuous fetal monitoring (CFM) was originally introduced in the 1950s, with technology developing further in the 1970s, and becoming routine in U.S. hospitals by the 1980s.
The original goal was to reduce:
Cerebral palsy
Perinatal death
Newborn morbidity
However, decades of data have shown that routine continuous fetal monitoring has not reduced rates of cerebral palsy or perinatal death.
Despite this, it has become the default standard of care in most U.S. hospitals — even for low-risk pregnancies.
Understanding the Fetal Heart Rate Tracing
When continuous monitoring is used, providers analyze several specific components:
1. Baseline Heart Rate
This is your baby’s average heart rate over a 10–30 minute window. A normal baseline typically falls between 110–160 beats per minute.
2. Variability
Variability refers to the small beat-to-beat fluctuations in heart rate. This is one of the most important indicators of how well-oxygenated your baby is.
Moderate variability = healthy oxygenation and nervous system function
Minimal or absent variability may indicate a baby who is under stress
A perfectly flat heart rate is not reassuring — healthy babies have natural variability.
3. Accelerations
Accelerations are brief increases in heart rate and are a good sign, indicating healthy oxygenation.
4. Decelerations
Decelerations are decreases in heart rate. There are three main types:
Early decelerations: Often caused by head compression and generally not concerning when variability is good.
Variable decelerations: Usually related to cord compression. Can become concerning if frequent, deep, or accompanied by worsening variability.
Late decelerations: The most concerning type. Often indicate issues with placental blood flow or oxygen delivery and require prompt attention.
Fetal Heart Rate Categories
Providers classify tracings into three categories:
Category One: Baby is well-oxygenated, stable, and thriving.
Category Two: A wide “gray zone.” Baby may be okay, but closer monitoring is needed.
Category Three: Baby is not tolerating labor and needs urgent intervention.
Category Two is often the most challenging to manage because it requires ongoing assessment and clinical judgment.
Two Options for Fetal Monitoring in Labor
1. Continuous Fetal Monitoring (CFM)
This involves constant monitoring of baby’s heart rate and contractions using external or internal monitors.
Benefits:
Continuous reassurance
Ability to assess variability
Ability to identify specific deceleration patterns
Earlier detection of fetal distress
Limitations:
Increased rates of:
C-sections
Operative vaginal deliveries
Medical interventions
Limited mobility (especially without wireless monitors)
Higher likelihood of cascade of interventions
Often leads to longer labors due to restricted movement
CFM can be life-saving and is absolutely appropriate for high-risk pregnancies, but evidence does not support its routine use for all low-risk labors.
2. Intermittent Auscultation (IA)
This method involves periodically listening to your baby’s heart rate using:
A fetoscope or pinard horn
A Doppler ultrasound device
Providers listen before, during, and after contractions at regular intervals (typically every 15–30 minutes).

What it assesses:
Baseline heart rate
Increases or decreases in heart rate
Benefits:
Increased freedom of movement
Upright labor positions
Shorter labors
Lower intervention rates
Low cost
Non-invasive
Limitations:
No continuous tracing
Cannot assess variability
Cannot classify types of decelerations
Potential to miss non-recurrent heart rate changes
Studies show that for low-risk pregnancies, intermittent auscultation does not increase rates of cerebral palsy or perinatal death compared to continuous monitoring.
There is a slight increase in neonatal seizures, but neonatal seizures are already extremely rare (well under 1%), making the absolute risk difference very small.

Why Isn’t Intermittent Auscultation Offered More Often?
In many U.S. hospitals, continuous monitoring is used routinely due to:
Hospital policies
Staffing models
Legal concerns
Standardization of care
Training differences
However, organizations like ACOG support offering intermittent auscultation for low-risk pregnancies as an evidence-based option.
Shared Decision-Making Matters
This is where informed choice becomes essential.
Some parents feel safest with continuous monitoring because they value constant reassurance. Others prioritize mobility, physiological labor, and lower intervention rates and prefer intermittent auscultation.
Neither choice is wrong.
The problem arises when people are never told there is a choice.
How to Advocate for Your Preferences
If you are low-risk and interested in intermittent auscultation:
Ask your provider directly if it’s available
Discuss hospital policies
Include it in your birth plan
Ask how transfers to continuous monitoring would be handled if risk status changes
If you prefer continuous monitoring:
Advocate for wireless or portable monitors
Ask about mobility-friendly options
Ask about upright labor positions even with monitors
The Takeaway
For high-risk pregnancies, continuous fetal monitoring is often the safest and most appropriate choice.
For low-risk pregnancies, both options are valid:
Continuous fetal monitoring offers constant data but increases intervention risk
Intermittent auscultation supports physiologic birth, mobility, and lower intervention rates
The goal is not to label one as “good” or “bad,” but to recognize that:
Evidence-based care includes choice.
You deserve to understand your options. You deserve informed consent. You deserve shared decision-making.
Prenatal Support Courses


Learn the science of pregnancy and birth to take the mystery of labor away! Understand why you are feeling what you feel, and learn strategies to confidently move through pregnancy and birth!
- 9h+ of Video
- Support Group
- Close Captioning


- 5 Workouts/Week
- Gym Workouts
- Self-Paced

Instructor
GINA
Workout on-demand with our prenatal fitness workout videos! Each workout is 30-40 minutes to follow along as you exercise at the same time!
- Birth Prep
- All Trimesters
- Mobility Work

Instructor
GINA
Find comfort and relief from pelvic girdle pain throughout your pregnancy and postpartum period! This program incorporates myofascial sling focused exercises to stabilize across the pelvic girdle joints.
- 3 Weeks
- On Demand Workout Videos to Follow