



Over the past decade, Roxanne and I have dedicated our careers to supporting pregnant women through pregnancy, birth, and postpartum recovery. Roxanne spent more than ten years as a labor and delivery nurse and now practices as a certified nurse midwife. I have supported women through birth as a birth doula, coaching everything from labor positioning to birth pushing positions, and through pregnancy and postpartum as a perinatal fitness trainer and co-founder of MamasteFit.
Together, we have attended hundreds, if not thousands, of births in person. We have also worked with thousands of women through our childbirth education courses, professional trainings, fitness programs, and workshops. Through those experiences, we have had the opportunity to observe labor unfold in many different ways and across many different birth settings.
One of the core values at MamasteFit is that we are always learning. We are constantly studying new research, exploring movement science, collaborating with other professionals, and reflecting on what we observe in real-world practice. It would be much easier to teach the exact same thing year after year. Changing your perspective can be uncomfortable, especially when you’ve spent years educating others on a topic.
But it is hard to ignore what you consistently see in practice.
Over the years, some of our beliefs about pelvic mechanics have remained the same. The pelvis moves. Position changes matter. Mobility matters. Birth is dynamic.
At the same time, there are several areas where our understanding has evolved significantly. Some concepts that we once emphasized heavily now seem less important. Other concepts that we barely discussed years ago have become central to how we teach birth preparation today.
In this blog, we’re sharing some of the biggest mindset shifts we’ve had regarding pelvic mechanics, how babies navigate the pelvis during labor, and what we now prioritize when preparing women for birth.
If you’re a birth professional, these concepts form the foundation of what we teach in our Pelvic Mechanics Workshop and Online Professional Course. If you’re currently pregnant, understanding these principles can also help you better understand why our prenatal fitness programs place such a strong emphasis on movement variability, pelvic mobility, and birth preparation exercises throughout pregnancy.
Shift #1: There Are Two Timelines in Birth
One of our first introductions to pelvic mechanics was through Spinning Babies after attending an in-person workshop in 2018. Their approach emphasized that when we are creating space within the pelvis, we need to consider where the baby is positioned. This concept introduced us to the idea that there is more than one process happening during labor and birth. At the time, this was a major shift in how we thought about labor positions because it connected maternal movement with the baby’s journey through the pelvis rather than focusing solely on the mother’s stage of labor.
Commonly, labor positions and pelvic mechanics are taught according to the phase of labor. In early labor, the focus is often on opening the inlet or top of the pelvis. In active labor, the focus shifts toward creating space through the midpelvis. Once someone begins pushing, the recommendation is frequently to focus on opening the outlet or bottom of the pelvis. While this framework can be helpful as an introduction to pelvic mechanics, it assumes that the baby’s journey through the pelvis is perfectly synchronized with the labor timeline. Over the years, we have found that this is not always the case.
There are actually two timelines occurring simultaneously during birth. The first timeline is the maternal labor timeline, which includes early labor, active labor, transition, and pushing. This timeline reflects what the mother’s body is experiencing, including changes in contraction intensity, contraction frequency, cervical dilation, and the overall progression of labor. This is typically the timeline we discuss in childbirth education classes and the one most care providers use when describing labor progress.
The second timeline is the baby’s journey through the pelvis. This is the timeline we consider when discussing pelvic mechanics. The baby must engage into the pelvic inlet, rotate through the midpelvis, and eventually extend beneath the pubic bone as they move through the outlet. While these events are occurring during the same birth experience, they do not necessarily happen in sync with the maternal labor timeline.
For example, a baby may already be deeply engaged in the pelvis during early labor. In that situation, spending all of your time focusing on inlet-opening positions may not be the most useful strategy because the baby may already be past that portion of the pelvis. Instead, positions that create space through the midpelvis may be more appropriate. On the other hand, another baby may still be trying to engage into the inlet during active labor. Even though labor has progressed into a later phase, inlet-opening positions may still be exactly what is needed to support progress.
One of the biggest mindset shifts we have had over the years is realizing that the pushing phase does not automatically mean the baby is navigating the outlet. In fact, when pushing begins, the baby is often still working through the midpelvis. Many babies do not reach the outlet until much later in the pushing phase. This helps explain why some women may spend a significant amount of time pushing before crowning occurs. The baby may still be rotating and navigating the middle portion of the pelvis rather than simply moving through the outlet. We frequently see birth education simplify pushing as “open the outlet,” but the reality is often much more complex than that.
This perspective has completely changed how we think about labor positions. Rather than selecting positions solely based on the phase of labor, we try to consider where the baby may be within the pelvis and what space needs to be created at that specific moment. Understanding that there are two timelines occurring simultaneously, but not always in sync, is one of the most important concepts in pelvic mechanics. It allows us to use labor positions more intentionally and adapt our approach based on the needs of both the mother and the baby throughout labor.
This concept is one of the foundations of our in-person Pelvic Mechanics Workshop and Online Professional Course. Rather than memorizing labor positions for each phase of labor, we teach professionals how to assess where baby may be within the pelvis and select positions based on the mechanics needed in that moment.
For pregnant readers, this is also why our prenatal fitness programs focus on developing movement options rather than mastering one “perfect” birth position. The more movement options you have available, the easier it is to adapt throughout labor as both timelines unfold.
Shift #2: The Inlet Has an Anterior and Posterior Inlet
When we were first introduced to pelvic mechanics, we learned that the pelvic inlet opens more with a posterior pelvic tilt, or what many people describe as tucking the tailbone under. This concept is based on the idea that a posterior pelvic tilt moves the sacral promontory, the junction between the sacrum and lumbar spine, backward, creating more front-to-back space within the pelvic inlet.
As a result, many of our early birth preparation exercises and labor positions focused on rounding through the back while maintaining wide knees. If our goal was to help a baby engage into the pelvis, we thought the answer was simple: posterior pelvic tilt and external rotation with abduction.
However, as our understanding of pelvic mechanics evolved through continuing education, mentorship with pelvic floor physical therapists, and years of observing labor unfold in real life, we realized the story was much more complicated than that.
One of the biggest mindset shifts we have had is recognizing that the entire pelvic inlet does not open with a single movement pattern. Different movement patterns create space in different portions of the inlet. In fact, the entire pelvis does not open with one movement, and even individual levels of the pelvis do not open with one movement.
Like, what?!
The pelvic inlet can be influenced by both anterior and posterior pelvic tilt, just in different ways.
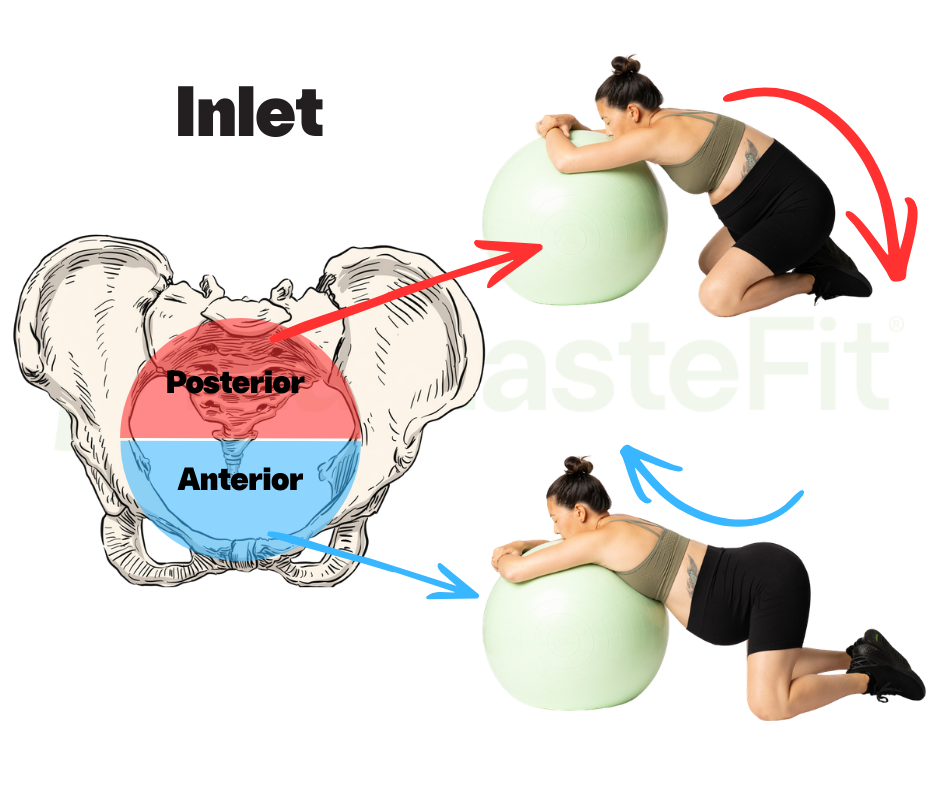
An anterior pelvic tilt changes the angle of the pubic bone, creating more space through the anterior portion of the inlet and potentially making it easier for a baby to slide behind the pubic bone as engagement occurs. An anterior pelvic tilt also tends to make hip external rotation more accessible because it changes the orientation of the femur within the hip socket. This can further contribute to opening through portions of the inlet.
A posterior pelvic tilt influences the inlet differently. By moving the sacral promontory posteriorly, it creates more space through the posterior aspect of the inlet. Rather than thinking of one movement as “the inlet opener,” we now think about how different movements influence different regions of the inlet.
This realization completely changed how we approach birth preparation and labor positioning. Instead of searching for one perfect position to open the inlet, we now focus on helping our clients access both anterior and posterior pelvic tilt. Often, alternating between these positions or creating a rocking motion through the pelvis may be more useful than holding a single posture for an extended period of time.
This perspective also helped us better understand why some of the classic “engagement positions” seem to work so well. For years, I was confused by positions like Walcher’s. If posterior pelvic tilt opens the inlet, why would a position that creates such a significant arch in the lower back help with engagement?
I was initially taught that because the hips are pushed into extension, Walcher’s ultimately creates a posterior pelvic tilt. However, when observing people in the position, most individuals appear to move into a fairly significant anterior pelvic tilt. Rather than viewing this as contradictory, it actually makes sense when we consider that an anterior pelvic tilt influences the pubic bone angle and can create more space through the anterior inlet.
This is why positions such as Walcher’s and Flying Cowgirl may be effective for some clients. They exaggerate anterior pelvic tilt and create space through the front of the inlet, while many of the more rounded and tucked positions create space through the back of the inlet. Both movement strategies may have value depending on what the baby and pelvis need in that moment.
Today, we spend much less time asking, “What is the best position to open the inlet?” and much more time asking, “Can this person move between anterior and posterior pelvic tilt?” Because ultimately, labor is dynamic. The pelvis is dynamic. And sometimes creating space is less about finding the perfect position and more about having access to multiple movement options.
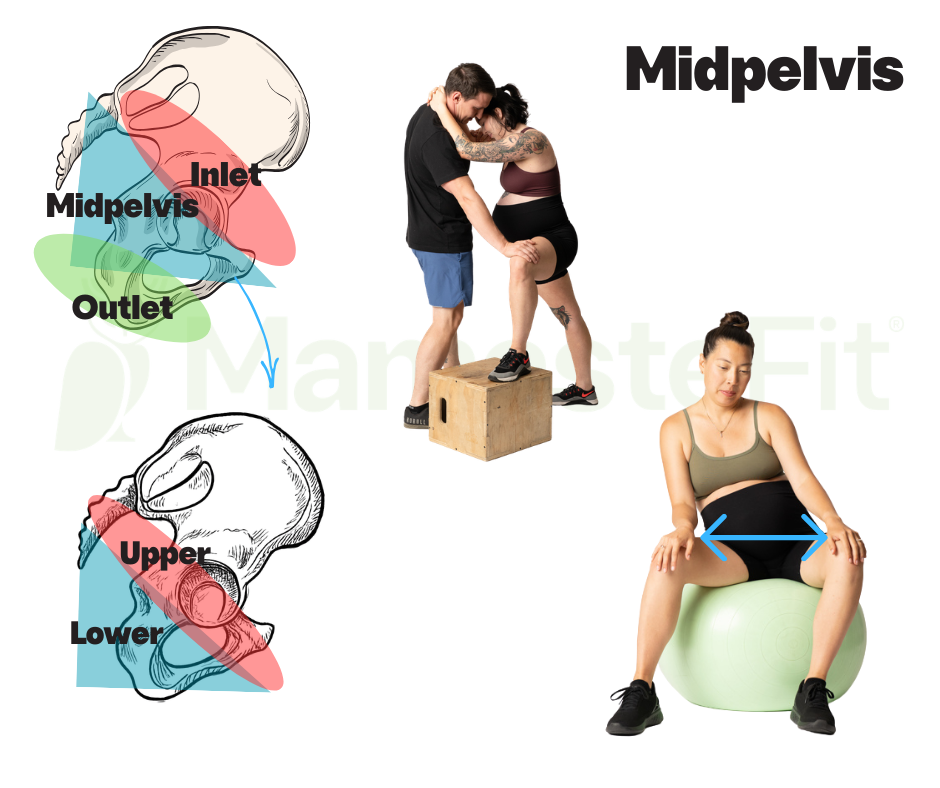
Shift #3: The Midpelvis Has Two Levels
Interestingly, this realization actually came before we understood that the inlet has both an anterior and posterior component. One of our earliest and biggest mindset shifts was recognizing that the midpelvis is not one single space. Instead, there are two distinct levels within the midpelvis that appear to influence different portions of baby’s rotational journey through the pelvis.
When we were first learning pelvic mechanics, we tended to think about the midpelvis as one area that opened and closed with specific positions. However, as we spent more time studying movement, observing births, and diving into concepts from the Postural Restoration Institute (PRI), we began to appreciate the triplanar movement that occurs through each half of the pelvis during normal human movement. Rather than thinking about the pelvis as one solid ring, we started viewing it as two pelvic halves that are constantly changing orientation as we walk, shift weight, squat, lunge, and move through daily life.
This was a huge “aha” moment for me.
The midpelvis appears to open through diagonal movement patterns that involve shifting weight into one leg or the other while alternating between open and closed hip positions. As weight shifts, one side of the pelvis rotates into a different orientation while the opposite side either rotates in the opposite direction or remains relatively neutral. These subtle positional changes can create space in different regions of the midpelvis and may help support the baby’s rotational journey.
The upper midpelvis tends to open more through non-stance positions in an open hip orientation. These positions often include hip external rotation, abduction, and anterior pelvic tilt. As this occurs, the upper portion of that side of the pelvis rotates forward, which may help create space for the baby to begin rotating as they move deeper into the pelvis. When you look at movements commonly used for engagement issues, such as portions of the Miles Circuit, exaggerated side-lying positions, or elevated lunges, many of these positions emphasize upper midpelvis opening mechanics. This may be one reason they can be helpful when a baby needs more room to begin rotating into an optimal position.
The lower midpelvis appears to open through almost the opposite movement pattern. These positions involve a stance leg in a more closed hip orientation, including internal rotation, adduction, and posterior pelvic tilt. Rather than creating space through the upper portion of the pelvis, these movements influence the lower half and may help create room beneath the pubic bone for the baby to complete rotation. This is why positions such as the side-lying release, hip shifts, and other internal rotation-focused movements may be helpful when a baby seems to be struggling to finish rotation during labor.
One of the biggest changes in our teaching has been realizing that labor is not simply about finding one position to open the midpelvis. Instead, it is often about the ability to move between upper and lower midpelvis mechanics. The pelvis is designed to alternate between these positions during movement, and labor may benefit from that same variability. While specific positions can be useful when addressing a labor stall or positional challenge, the larger goal is helping women develop the ability to access both movement patterns.
Pregnancy NEEDS More Pelvic Internal Rotation as a Part of Birth Prep
This realization has also influenced how we design our prenatal fitness programs and birth preparation exercises. Many women enter pregnancy with common postural tendencies that make lower midpelvis opening mechanics more difficult to access. Internal rotation, adduction, and weight shifting into a stance leg are often movement patterns that have become limited long before labor begins. This is one of the reasons hip shifts have become such a foundational component of our birth preparation approach. Improving access to these movement patterns can be a game changer not only for birth preparation, but also for pelvic stability, pelvic floor tension management, and overall comfort throughout pregnancy.
Rather than asking whether the midpelvis is open or closed, we now ask a different question: can this person access both the upper and lower levels of the midpelvis and move between them when needed? That shift in perspective has completely changed how we approach birth preparation and labor positioning.
Applying Midpelvis Mechanics to Birth Preparation
Understanding upper and lower midpelvis mechanics has completely changed how we approach birth preparation. Rather than focusing on stretching one muscle or practicing one labor position, we focus on helping our clients develop the movement options needed to create space throughout the pelvis and adapt to the changing demands of labor.
For pregnant readers, this is exactly why our prenatal fitness programs and Birth Prep Circuit include exercises such as hip shifts, lunges, step-ups, single-leg strengthening, and pelvic mobility work. These exercises are designed to improve your ability to access different regions of the pelvis so you have more movement options available when labor begins.
For birth professionals, understanding the difference between upper and lower midpelvis mechanics can completely change how you approach labor support. Instead of simply recommending positions based on the stage of labor, you can begin selecting movements and positions based on where the baby may be navigating within the pelvis and what type of space needs to be created. We teach these concepts in much greater detail in our in-person Pelvic Mechanics Workshop and Online Professional Course, where we break down the biomechanics, assessments, labor positions, and hands-on techniques we use to support labor progress.
Shift #4: Birth Pushing Positions Are More Than "Knees In, Ankles Out"
Another huge shift for us has been how we think about opening the pelvic outlet during pushing. Over the years, there have been several changes in our understanding of outlet mechanics, and many of them stem from observing what clients naturally do during labor versus what we were originally taught to coach.
One of the most significant realizations is that “knees in, ankles out” may not always be the best approach for every person during pushing.
If we go back to the concept of the two timelines discussed earlier, the baby is not always in the outlet when pushing begins. In fact, most babies are still navigating portions of the midpelvis when the pushing phase starts. This means that while the labor timeline has entered the pushing phase, the baby’s timeline may still involve rotation through the pelvis.
When we observe clients pushing without extensive coaching, many naturally choose asymmetrical positions rather than symmetrical knees-in positions. They may gravitate toward lunges, side-lying positions, staggered stances, or positions that allow them to shift their weight from one side to the other. Clinically, we have often observed that when a baby appears to be hung up in the pelvis during pushing, introducing a movement such as a hip shift, lunge, or asymmetrical position can sometimes help the baby continue rotating and begin descending more effectively. Frequently, this is when we see a baby begin to crown.
This has led us to question whether the best pushing position is always the one that maximizes outlet dimensions or whether, in some situations, creating space through the midpelvis may be more important because the baby is still navigating that region of the pelvis.
Pushing Does NOT = Open the Outlet
Another shift in our thinking is how we understand internal rotation. Traditionally, outlet-opening positions are often taught as positions that place the hips into internal rotation. However, we now think it is more useful to consider where the movement is actually occurring. In many situations, the goal is not simply rotating the femur inward. The goal is influencing the orientation of the pelvis itself.
This is one reason why all-fours positions have become increasingly interesting to us. In quadruped, the femurs drive backward into the hip sockets, which may help influence pelvic orientation and create more space through the posterior outlet. Interestingly, the legs themselves may appear relatively neutral or even externally rotated, yet the pelvis can still be positioned in a way that supports outlet mechanics. This is a much more subtle concept than simply looking at the position of the knees and feet, and it is something we spend significant time exploring in our in-person Pelvic Mechanics Workshop and Online Professional Course.
Do You Really NEED To Open the Outlet?
Perhaps the biggest shift, however, is recognizing that the outlet is largely a soft tissue challenge rather than a bony challenge. While bony dimensions certainly matter, much of what the baby encounters at the outlet involves the pelvic floor, connective tissues, surrounding musculature, and the client’s ability to relax and yield.
Because of this, we have become less focused on aggressively trying to maximize outlet dimensions and more focused on helping clients find positions where they can relax, respond to contractions, and effectively work with their body. In many cases, restorative positions such as side-lying or even semi-reclined positions may feel significantly better than highly active positions. Rather than viewing this as a problem, we now see it as an important part of the process. A position that allows a client to release tension and yield to the demands of labor may be more valuable than a position that theoretically creates a few extra millimeters of space.
Does Opening ONLY the Outlet Cause Shoulder Issues?
One of the newest questions we have been exploring involves what happens after the baby’s head reaches the outlet. During engagement and rotation, only the baby’s head is navigating the pelvis. Once crowning begins, however, the baby’s head may be moving through the outlet while the shoulders and body are still navigating the inlet and midpelvis.
This raises an interesting question: if we focus exclusively on opening the outlet, are we considering what the rest of the baby’s body still needs to navigate? This question came up during a discussion with several midwives at one of our Pelvic Mechanics Workshops. Some shared observations that made us wonder whether there are situations where continuing to emphasize aggressive outlet-opening strategies after crowning begins may not always be the most helpful approach.
To be clear, we do not have definitive answers here. Instead, this is one of the areas where our thinking continues to evolve. What we do know is that birth is more complex than simply opening one level of the pelvis at a time. The baby is navigating a three-dimensional space, the pelvis is constantly adapting, and sometimes the most effective strategy is not forcing a particular position but helping the client find movement, comfort, relaxation, and adaptability throughout the pushing process.
Learning How to Apply Pelvic Mechanics During Labor
Understanding pelvic mechanics on paper is very different from knowing how to apply these concepts during a real labor. This is where observation, assessment, and experience become so valuable.
For birth professionals, our in-person Pelvic Mechanics Workshop and Online Professional Course go beyond memorizing labor positions. We teach you how to assess movement patterns, identify where a baby may be navigating within the pelvis, and choose positions based on the needs of the client and baby in front of you.
For pregnant clients, our prenatal fitness programs and Birth Prep Circuit are designed to help you build these movement options long before labor begins. Rather than practicing one “perfect” pushing position, you’ll develop strength, mobility, pelvic awareness, and movement variability so you have more options available when labor unfolds in its own unique way.
Shift #5: You Can Train for Birth... But You Cannot Guarantee an Outcome
Another significant shift in our perspective over the years is understanding what it actually means to prepare for birth.
When many people hear “birth preparation,” they assume that if they do all the right things, they will get the birth they want. If they take the classes, do the exercises, practice the positions, and check all the boxes, then a specific birth outcome should follow. And if the birth does not go according to plan, it can be easy to feel like they missed something or did not prepare enough.
Over the years, we have learned that birth does not work that way.
We cannot guarantee a specific birth experience, but we can absolutely stack the cards in our favor.
Birth preparation is about creating the conditions for an easier labor and birth. It is about improving movement options within the pelvis, reducing unnecessary tension, supporting pelvic floor function, encouraging fetal positioning, building confidence, and developing the ability to adapt throughout labor. None of these things guarantee a specific outcome, but they can help create an environment that supports physiologic birth and makes it easier to respond to whatever labor presents.
We also now recognize that effective birth preparation is multifactorial. It is not just physical preparation. It involves choosing a birth team that can provide expertise while respecting your autonomy and preferences. It involves education so you understand your options and can make informed decisions throughout pregnancy and labor. It involves developing confidence in your ability to navigate the unexpected. And yes, it involves physical preparation, but that preparation is about much more than doing a few deep squats at the end of pregnancy.
Physical preparation means improving your ability to move. It means learning how to access different movement patterns throughout the pelvis. It means developing strength, mobility, balance, coordination, and the ability to transition between positions with ease. The more movement options you have available, the more options you may have available during labor.
This philosophy has completely shaped how we design our prenatal fitness programs. Rather than giving clients a short list of birth prep exercises to perform occasionally, we integrate these concepts into a comprehensive strength and movement program throughout pregnancy. Every workout is designed to improve movement capacity, pelvic mobility, strength, and body awareness while preparing for the demands of labor, birth, and postpartum recovery.
Whether you prefer self-paced strength training or follow-along video workouts, our prenatal fitness programs guide you through pregnancy week by week with workouts designed specifically for your stage of pregnancy. Our goal is not to promise a particular birth outcome. Our goal is to help you build the movement options, confidence, and physical capability that may support an easier and more comfortable pregnancy and birth experience.
These concepts have also changed how we educate birth professionals. Too often, birth preparation begins once labor starts. However, many of the movement patterns we rely on during labor can be difficult to access for the very first time during an intense contraction. It is challenging to teach someone how to perform a hip shift, access internal pelvic rotation, or coordinate a complex movement pattern in the middle of labor if they have never experienced those movements before.
This is why we believe birth preparation starts long before labor begins. Whether you are supporting yourself through pregnancy or supporting clients professionally, there is tremendous value in building movement options ahead of time so they are available when they are needed most.
Conclusion: Our Understanding of Birth Continues to Evolve
There are many ways our approach to pelvic mechanics, birth preparation, and labor support has evolved over the years. Every continuing education course, every conversation with another professional, every client interaction, and every birth we attend adds another layer to our understanding.
Some of the concepts we once taught as simple rules have become much more nuanced. We now appreciate that the inlet has both anterior and posterior components. We recognize that the midpelvis is more complex than a single level. We spend less time searching for the perfect outlet-opening position and more time considering relaxation, adaptability, and where the baby is actually navigating within the pelvis. Most importantly, we have learned that labor is not a rigid sequence of positions but a dynamic process that often requires constant adjustment.
This growth has influenced everything we do at MamasteFit. It has shaped our prenatal fitness programs, our childbirth education courses, our Birth Prep Circuit, and our professional trainings. The exercises we program today are different than they were five years ago. The labor positions we teach have evolved. Even the way we explain pelvic mechanics continues to change as we gain new insights and observations.
What has not changed is our commitment to continuing to learn. We believe that supporting pregnancy and birth requires curiosity, humility, and a willingness to adapt when new information challenges old assumptions.
If you are pregnant and looking for guidance, our prenatal fitness programs are built around these principles and designed to help you prepare for birth through strength training, mobility work, pelvic preparation, and movement education. If you are a birth professional, our in-person Pelvic Mechanics Workshop and Online Professional Course dive much deeper into these concepts and teach you how to apply them to real clients and real births.
The more we learn, the more we realize that birth is not about finding one perfect position, one perfect exercise, or one perfect approach. It is about developing options, understanding movement, and learning how to adapt throughout the process. And that is exactly what we hope to help you do.